


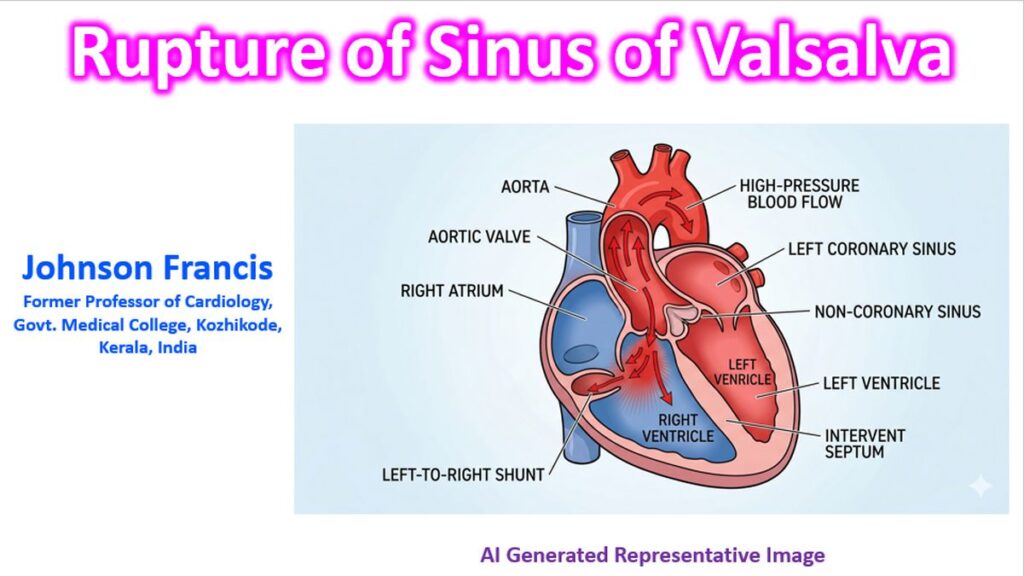

Rupture of the Sinus of Valsalva (RSOV) is a rare but clinically significant clinical event, usually involving a deficiency in the aortic media. It typically presents as a thin-walled, windsock-like aneurysm that eventually ruptures into an adjacent cardiac chamber, creating a significant left-to-right shunt.
1. Pathophysiology and Anatomy
Sinus of Valsalva consists of three anatomical dilatations of the aortic root: the right, left, and non-coronary sinuses.
- Origin: Most RSOVs are congenital, caused by a lack of continuity between the aortic media and the annulus fibrosus of the aortic valve.
- Site of Rupture:
- Right Coronary Sinus (~70–80%): Usually ruptures into the Right Ventricle (RV).
- Non-Coronary Sinus (~10–20%): Usually ruptures into the Right Atrium (RA).
- Left Coronary Sinus (<5%): Rarely ruptures, but may open into the Left Atrium or pericardium.
2. Clinical Presentation
SOV aneurysm often remains asymptomatic until the third or fourth decade of life unless a sudden, large rupture occurs.
- Acute Rupture: Sudden onset of severe chest pain, dyspnea, and rapidly progressing heart failure.
- Physical Exam: A classic continuous “machinery” murmur is heard, similar to a PDA but usually louder at the lower left sternal border rather than the infraclavicular area.
- Pulse: Wide pulse pressure and “water-hammer” pulses due to the rapid runoff of blood from the aorta into a lower-pressure chamber.
3. Associated Conditions
It is frequently associated with other congenital cardiac defects:
- Ventricular Septal Defect (VSD): Specifically the supracristal (subpulmonic) type, seen in up to 50% of cases.
- Bicuspid Aortic Valve: Present in about 10% of patients.
- Aortic Regurgitation: Often develops due to the lack of support for the aortic leaflets or the “Venturi effect” of the shunt pulling the leaflet down.
4. Diagnosis
- Echocardiography: Transthoracic (TTE) and Transesophageal (TEE) are the gold standards. Color Doppler reveals the continuous high-velocity jet. Windsock appearance in RVOT is characteristic.
- Cardiac MRI/CT: Excellent for defining the anatomy and measuring the size of the aneurysm if echo windows are suboptimal.
- Cardiac Catheterization: Primarily used to quantify the shunt (Qp/Qs) and assess the coronary arteries before surgical repair.
Continuous Murmurs: Differential Diagnosis
Since RSOV, PDA, and Coronary Artery Fistula (CAF) all produce continuous murmurs, the “spot-the-difference” lies primarily in the location of maximal intensity and the timing of the peak.
| Feature | Rupture of Sinus of Valsalva (RSOV) | Patent Ductus Arteriosus (PDA) | Coronary Artery Fistula (CAF) |
| Maximal Intensity | Lower left sternal border or xiphoid area. | Left infraclavicular area (Gibson’s area). | Variable; often over the lower sternum or right side (depends on the drainage site). |
| Peak Timing | Peaks in late systole/early diastole (when the pressure gradient is highest). | Peaks at the second heart sound (S2). | Often has a crescendo-decrescendo quality in both phases. |
| Classic Description | “Washing machine” or “Machinery” murmur; very superficial sounding. | Classic “Machinery” murmur. | “To-and-fro” or continuous; may be softer than RSOV. |
| Pulse Pressure | Very wide (rapid runoff into RV/RA). | Wide (runoff into Pulmonary Artery). | Usually normal to slightly wide. |
Clinical Pearls
- Superficial Nature: While all three are continuous, the RSOV murmur sounds “closer to the ear” because the rupture often occurs into the right-sided chambers which are right under the chest wall.
- Postural Variation: Unlike a venous hum (another continuous murmur differential), these murmurs do not disappear when the patient lies flat or turns their head.
- The VSD Clue: If you see a patient with a known VSD who suddenly develops a loud, new continuous murmur and heart failure, RSOV is the diagnosis until proven otherwise.
5. Management
Once ruptured, the prognosis is poor without intervention, typically leading to death from heart failure within one year.
- Surgical Repair: The traditional treatment involving excision of the “windsock” and patch closure (usually via a double approach through both the aorta and the receiving chamber).
- Percutaneous Closure: In selected cases where the anatomy is favorable (e.g., adequate margins from the coronary ostia and aortic valve), Amplatzer duct occluders or similar devices are increasingly used.