



In clinical electrophysiology and cardiac pharmacodynamics, calcium (Ca2+) currents serve as the fundamental bridge between electrical excitation and mechanical contraction. The two primary voltage-gated calcium channels expressed in the human heart—L-type (Long-lasting) and T-type (Transient)—dictate entirely different aspects of cardiac rhythm, conduction, and inotropy.
The Master Electrophysiological Comparison
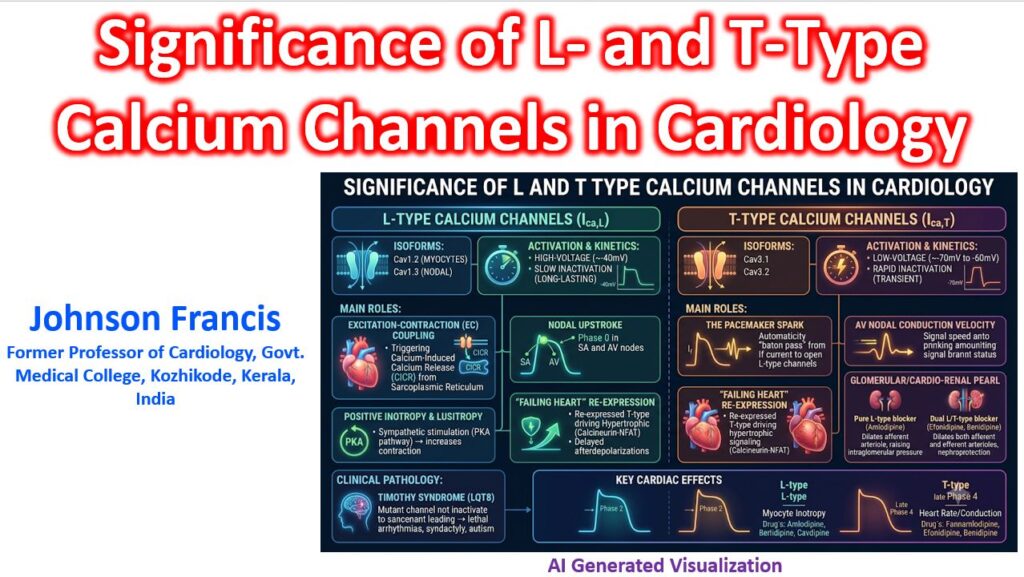
| Feature | L-Type Channels (ICa,L) | T-Type Channels (ICa,T) |
| Primary Isoforms | Cav1.2 (myocytes), Cav1.3 (nodal) | Cav3.1, Cav3.2 |
| Activation Threshold | High-voltage (≈ -40 mV ) | Low-voltage (≈ -70 mV to -60 mV) |
| Inactivation Kinetics | Slow (Long-lasting opening) | Rapid (Transient opening) |
| Healthy Distribution | Ubiquitous (Atria, Ventricles, Nodes, Purkinje) | Restricted (SA node, AV node, Purkinje fibers) |
| Action Potential Role | Phase 2 (Myocytes); Phase 0 (Nodal cells) | Late Phase 4 (Pacemaker depolarization slope) |
| Primary Function | Excitation-Contraction (EC) Coupling; Nodal upstroke | Automaticity spark; AV nodal conduction velocity |
| Classic Pharmacology | Dihydropyridines, Verapamil, Diltiazem | Efonidipine, Benidipine (Mibefradil – historical) |
1. L-Type Channels (ICa,L): The Drivers of Inotropy
The L-type channel is the quintessential “cardiac workhorse.” Because it requires a relatively strong depolarization to open (-40 mV), it acts as an amplifier rather than an initiator of electrical activity.
- Excitation-Contraction (EC) Coupling: In working atrial and ventricular myocytes, the fast sodium upstroke (Phase 0) brings the cell to the threshold required to open L-type channels. The resulting influx of Ca2+ during Phase 2 (the plateau) is physically too small to cause myofibrillar contraction on its own; instead, it serves as the obligatory trigger for Calcium-Induced Calcium Release (CICR) via Ryanodine Receptor 2 (RyR2) on the sarcoplasmic reticulum.
- Nodal Phase 0 Upstroke: Because the Sinoatrial (SA) and Atrioventricular (AV) nodes largely lack fast voltage-gated Na+ channels, their depolarization relies entirely on ICa,L. Therefore, Class IV antiarrhythmics (Verapamil, Diltiazem) slow AV nodal conduction by degrading the slope of this specific Phase 0.
- Autonomic Sensitivity: The α1 subunit of the Cav1.2 channel is the primary downstream target of β1-adrenergic stimulation. Phosphorylation via the cAMP/PKA pathway dramatically increases the channel’s open probability, providing the cellular basis for sympathetic positive inotropy and lusitropy.
- Clinical Pathology: Gain-of-function mutations in the CACNA1C gene (encoding Cav1.2) result in Timothy Syndrome (LQT8)—a lethal, multi-systemic form of Long QT characterized by syndactyly, autism, and malignant ventricular tachyarrhythmias caused by failure of the channel to properly inactivate.
2. T-Type Channels (ICa,T): The Pacemaker Spark
If the L-type channel is the heavy machinery, the T-type channel is the ignition switch. Because it activates at much more negative resting potentials (-70 mV), it operates in the voltage “dead zone” where L-type channels are fully shut.
- The Baton Pass of Automaticity: In the SA node, spontaneous Phase 4 diastolic depolarization is initiated by the hyperpolarization-activated “funny current” (If). As If drags the membrane voltage up to roughly -60 mV, ICa,T switches on. This transient calcium surge provides the vital push to reach -40 mV, successfully handing the baton over to the L-type channels to trigger Phase 0.
- The “Failing Heart” Re-expression: In healthy adult human ventricular myocytes, T-type channels are functionally silenced. However, under conditions of chronic pathological stress (eccentric/concentric hypertrophy, post-infarct remodeling, or HFrEF), the heart executes a reversion to the fetal gene program. Ventricular ICa,T is robustly re-expressed. This influx drives abnormal calcineurin-NFAT hypertrophic signaling pathways and loads the cytosol with excess calcium during diastole, lowering the threshold for Delayed Afterdepolarizations (DADs).
- The Glomerular/Cardio-Renal Pearl: Standard dihydropyridines (e.g., Amlodipine) act almost exclusively on L-type channels. In the kidney, L-type channels sit on the afferent arteriole, while T-type channels sit on the efferent arteriole. Pure L-type blockade dilates the afferent side, which can inadvertently raise intraglomerular hydrostatic pressure and worsen microalbuminuria. Dual L/T-type blockers (such as Efonidipine or Benidipine) dilate both the afferent and efferent arterioles simultaneously, offering superior nephroprotection in hypertensive nephropathy and cardioprotection in hypertensive cardiomyopathy.
Clinical Synthesis
When looking at surface electrocardiography or managing hemodynamics:
- Manipulating L-type alters the PR interval (AV nodal conduction), the QT interval (ventricular action potential duration), and left ventricular stroke volume.
- Manipulating T-type primarily alters the R-R interval (sinus node firing rate) and dictates the microvascular tone of peripheral and renal capillary beds.