


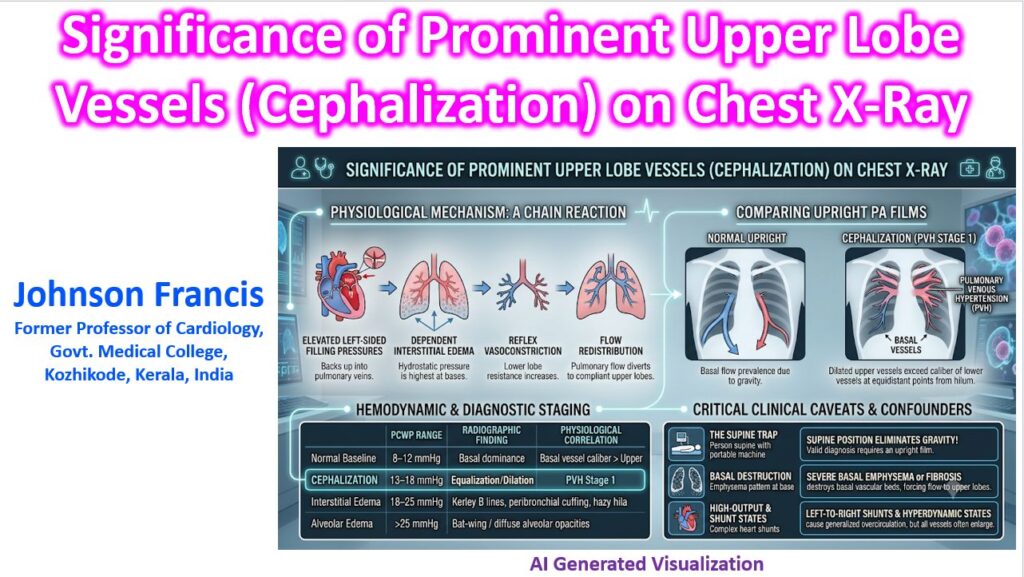

Prominent upper lobe vessels on a chest X-ray—a phenomenon clinically termed cephalization (or redistribution)—is the hallmark radiographic sign of pulmonary venous hypertension (PVH).
In a healthy, upright individual, gravity causes blood to flow predominantly to the lung bases. Consequently, lower lobe vessels are normally significantly larger and more numerous than the nondependent upper lobe vessels. When you see prominent, dilated upper lobe vasculature exceeding the caliber of the lower lobe vessels at equidistant points from the hilum, it signals an upward shift in pulmonary perfusion.
Physiological Mechanism
The classic pathophysiology follows a strict hemodynamic chain reaction:
- Elevated Left-Sided Filling Pressures: Whether due to left ventricular systolic/diastolic dysfunction, mitral valve disease, or volume overload, elevated left atrial pressure backs up directly into the valveless pulmonary veins.
- Dependent Interstitial Edema: Because hydrostatic pressure is naturally highest at the lung bases due to gravity, fluid first leaks into the basal interstitium when pulmonary capillary wedge pressure (PCWP) rises.
- Reflex Vasoconstriction: This perivascular interstitial edema compresses the basal pulmonary vessels and triggers localized hypoxic/hypercapnic vasoconstriction in the lower lobes.
- Flow Redistribution: With vascular resistance spiking at the bases, pulmonary arterial flow takes the path of least resistance, diverting upward to the normally underperfused, highly compliant upper lobes.
Hemodynamic & Diagnostic Staging
Cephalization acts as an indirect, visual manometer for estimating PCWP in acute or worsening decompensation:
| PCWP Range | Radiographic Finding | Physiological Correlation |
| 8–12 mmHg | Normal baseline | Basal vessel caliber > Upper lobe caliber |
| 13–18 mmHg | Cephalization | Equalization or upper lobe dilation (PVH stage 1) |
| 18–25 mmHg | Interstitial Edema | Kerley B lines, peribronchial cuffing, hazy hila |
| > 25 mmHg | Alveolar Edema | Classic “bat-wing” or diffuse alveolar opacities |
Critical Clinical Caveats
Before using cephalization to drive clinical decisions, three major confounding variables must be ruled out:
- The Supine Trap: Cephalization can only be reliably diagnosed on an erect (PA or AP) film. When a patient is supine—such as in portable ICU chest films—the hydrostatic gravitational gradient between the apex and base is eliminated. Perfusion naturally equalizes, creating pseudo-cephalization.
- Basal Destruction (Shunting of Flow): Severe basal emphysema or extensive lower-lobe fibrosis mechanically destroys basal vascular beds. This forces blood to the upper lobes regardless of left heart pressures, mimicking cardiac redistribution.
- High-Output & Shunt States: Left-to-right intracardiac shunts (like ASDs or VSDs) or systemic hyperdynamic states (thyrotoxicosis, severe anemia, AV fistulas) cause generalized pulmonary hyperperfusion. While upper lobe vessels enlarge, basal vessels usually dilate proportionally.