


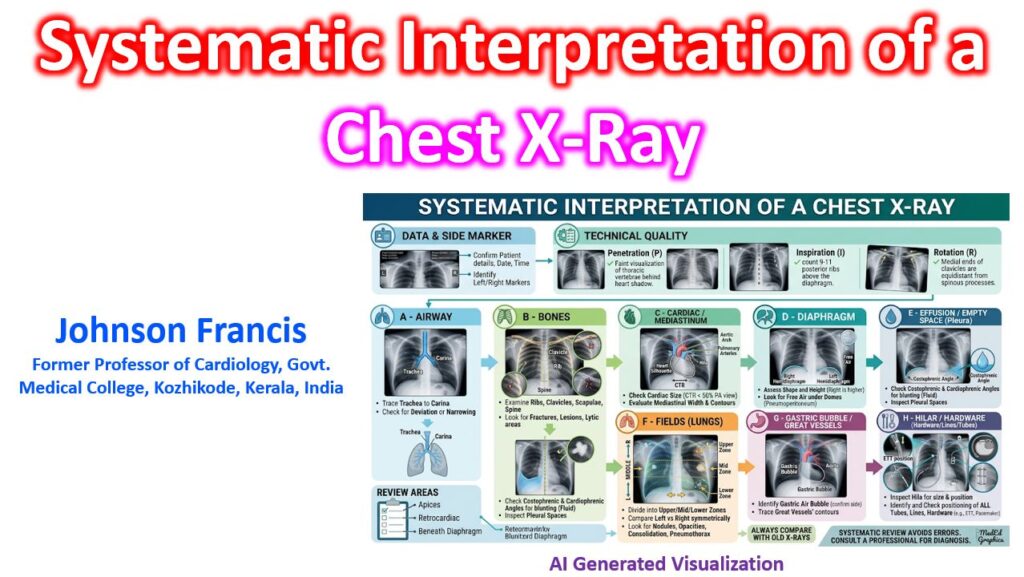

A rigorous, reproducible system is essential for avoiding “satisfaction of search” — stopping your review of the chest X-ray once you find an obvious abnormality and missing secondary findings. The universally accepted framework in clinical practice relies on a strict pre-read quality check followed by the ABCDEFGH sequence.
1. The Pre-Read Check (RIP)
Before interpreting pathology, confirm the technical quality of the film. A poor-quality image can easily mimic or mask disease.
- Rotation: The thoracic spinous processes should align exactly midway between the medial ends of the clavicles. Rotation significantly alters the apparent heart size and lung density.
- Inspiration: A good inspiratory effort brings the diaphragm down to the level of the 5th-6th anterior ribs, or 8th-10th posterior ribs. Poor inspiration mimics basal consolidation and artificially enlarges the cardiac silhouette.
- Penetration (Exposure): You should be able to faintly see the lower thoracic vertebral bodies through the cardiac shadow. Over-penetrated films black out subtle lung markings; under-penetrated films obscure the lung bases and retrocardiac space. Upper thoracic spines are clearly seen through tracheal air column.
2. The ABCDEFGH Sequence
A: Airway
Trace the trachea down to the carina. It should be central or slightly displaced to the right by the aortic arch. Check for narrowing, foreign bodies, or deviation. Tracheal deviation suggests a mediastinal shift, often driven by tension pneumothorax, large effusion, or massive atelectasis. Ensure the mainstem bronchi branch at a normal angle (usually <90 degrees).
B: Bones & Soft Tissue
Scan the ribs, clavicles, scapulae, and the visible spine.
- Pro tip: Trace each rib individually from posterior to anterior to avoid missing subtle or hairline fractures.Look for lytic/sclerotic lesions or step-offs. In the soft tissues, check for subcutaneous emphysema, surgical clips, or abnormal masses.
C: Cardiac Silhouette & Mediastinum
Evaluate the heart size. On a PA film, the cardiothoracic ratio (CTR) should be strictly <50%.
- Right border: Formed by the right atrium.
- Left border: Formed by the left ventricle and left atrial appendage.
- Mediastinum: Check the aortic knob, the pulmonary bay, and the hilum (the left hilum normally sits slightly higher than the right). Widening of the mediastinum (>8 cm) is a red flag for aortic dissection or significant lymphadenopathy.
D: Diaphragm
The right hemidiaphragm is typically 1-3 cm higher than the left. Check the contour—it should be a smooth, continuous dome. Look closely for free air under the diaphragm (pneumoperitoneum), appearing as a thin radiolucent crescent, which requires immediate surgical attention.
E: Effusions (Costophrenic Angles)
Inspect the lateral costophrenic and cardiophrenic angles. They should be sharply pointed. Blunting indicates pleural effusion or pleural thickening. Note that it typically takes 200-300 mL of fluid to blunt the angle on a PA film, whereas a lateral film can reveal as little as 50 mL.
F: Fields (Lungs)
Divide the lungs into upper, mid, and lower zones. Compare left to right symmetrically, scanning in a zig-zag pattern.
- Check for consolidation, masses, or solitary pulmonary nodules.
- Look for interstitial patterns, such as reticular opacities or Kerley B lines at the bases.
- Follow the vascular markings all the way to the periphery. If they stop abruptly, look closely for a thin pleural line indicating a pneumothorax.
- In the setting of elevated left-sided filling pressures, look for cephalization of flow (dilation of upper lobe vessels).
G: Gastric Bubble
Locate the radiolucent gastric bubble under the left hemidiaphragm. Ensure it is in the correct anatomical position (absent or on the right in situs inversus). Check the distance between the lung base and the bubble; abnormal separation can suggest a subpulmonic effusion or gastric wall pathology.
H: Hardware & Tubes
Methodically identify all lines, tubes, and devices, ensuring correct placement and integrity.
- Tubes/Lines: Endotracheal tubes (tip should be 3-5 cm above the carina), central venous catheters (tip at the cavoatrial junction), and NG tubes (tip below the diaphragm).
- Devices: Pacemakers and ICDs (check lead continuity, fractures, and positioning), sternal wires, and prosthetic heart valves.