



Tachycardia-Induced Cardiomyopathy (TIC)—often referred to as Arrhythmia-Induced Cardiomyopathy—is a unique clinical entity where persistent or frequent tachyarrhythmias lead to significant ventricular dysfunction. The hallmark of TIC is its potential for partial or complete reversibility once the heart rate is controlled or the rhythm is restored.
Pathophysiology
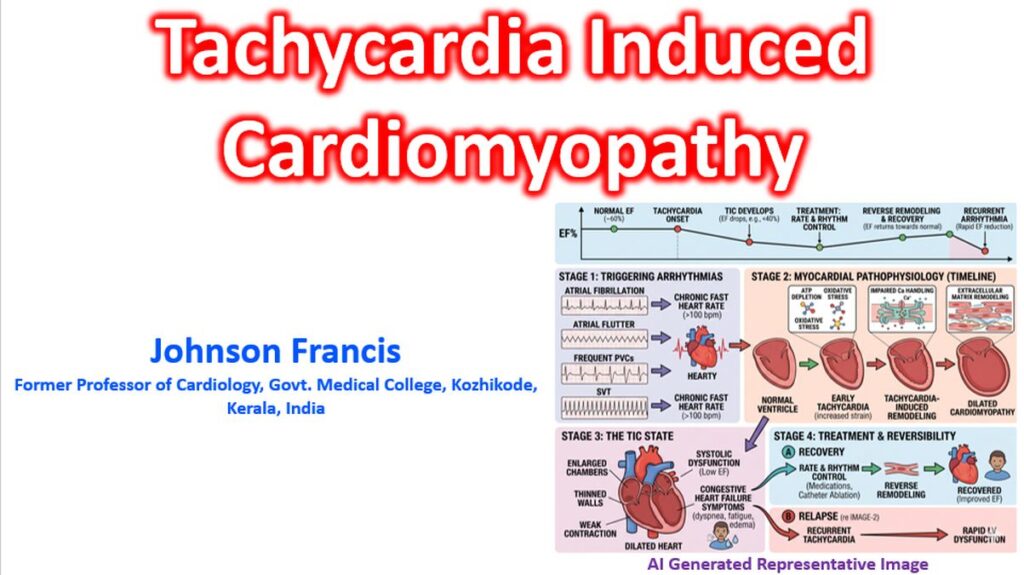
The exact mechanisms are complex, but cellular and structural changes typically include:
- Myocardial Energetics: Depletion of high-energy phosphates (ATP and phosphocreatine) and reduced mitochondrial efficiency.
- Calcium Handling: Abnormalities in sarcoplasmic reticulum calcium-ATPase (SERCA2a) activity, leading to impaired excitation-contraction coupling.
- Structural Remodeling: Myocyte elongation, loss of myofibrils, and increased extracellular matrix collagen deposition, though notably with less prominent fibrosis than other dilated cardiomyopathies (which explains the potential for recovery).
- Ischemia: Reduced subendocardial blood flow and coronary flow reserve due to shortened diastole.
Common Clinical Triggers
While any sustained tachycardia can cause TIC, the most frequent culprits include:
- Atrial Fibrillation (AFib): The most common cause, particularly when the ventricular response is poorly controlled.
- Atrial Flutter: Especially 2:1 conduction leading to sustained rates of ~150 bpm.
- Frequent Premature Ventricular Contractions (PVCs): Typically requires a high burden (often >15–20% of total beats), though TIC has been observed with burdens as low as 10%.
- Supraventricular Tachycardias (SVT): Including permanent junctional reciprocating tachycardia (PJRT) and WPW syndrome.
- Incessant Ventricular Tachycardia: Often originating from the outflow tracts.
Diagnostic Criteria
TIC is often a diagnosis of exclusion or confirmed retrospectively. Key indicators include:
- LVEF Reduction: Dilated or non-dilated LV with reduced ejection fraction.
- Persistent Tachycardia: Usually defined as a heart rate >100 bpm for a significant portion of the day.
- Absence of Other Causes: No significant CAD, valvular disease, or primary myopathy that fully explains the degree of dysfunction.
- Recovery: Improvement in LVEF (usually within 1–6 months) following effective rate or rhythm control.
Management Strategies
The primary goal is the “normalization” of the heart rate or restoration of sinus rhythm.
| Approach | Interventions |
| Rhythm Control | Catheter Ablation: Highly effective for PVCs, AFib, or SVTs. Ablation is often preferred over long-term Pharmacotherapy in TIC due to higher cure rates. |
| Rate Control | Pharmacotherapy: Beta-blockers, non-dihydropyridine calcium channel blockers (Verapamil/Diltiazem), or Digoxin. |
| Advanced Options | “Ablate and Pace”: AV node ablation followed by permanent pacemaker/CRT implantation if pharmacological rate control fails in AFib. |
| Heart Failure Rx | Standard GDMT (ACEi/ARB/ARNI, MRA, SGLT2i) should be initiated while waiting for recovery. |
Key Clinical Considerations
- The “Double Hit”: Tachycardia can be the primary cause of cardiomyopathy, or it can exacerbate an underlying substrate (e.g., a patient with mild hypertensive heart disease who develops AFib). These two varieties have been called as ‘Pure’ and ‘Impure’ tachycardia induced cardiomyopathy.
- Recurrence Risk: Even after LVEF recovery, these patients remain at high risk for “tachycardia-induced” failure if the arrhythmia recurs. There is often a “memory” in the myocardium where the LVEF can drop much more rapidly during a second episode.
- PVC Morphology: PVCs originating from the RVOT or LVOT are common targets for ablation; identifying the origin via 12-lead ECG is critical for planning intervention.