



In the Cardiac Care Unit (CCU), some ECG patterns represent immediate threats to life, often preceding sudden cardiac arrest or profound hemodynamic collapse. While some are obvious, others are subtle “wolf in sheep’s clothing” patterns.
Here are five potentially lethal ECG patterns every clinician must recognize instantly:
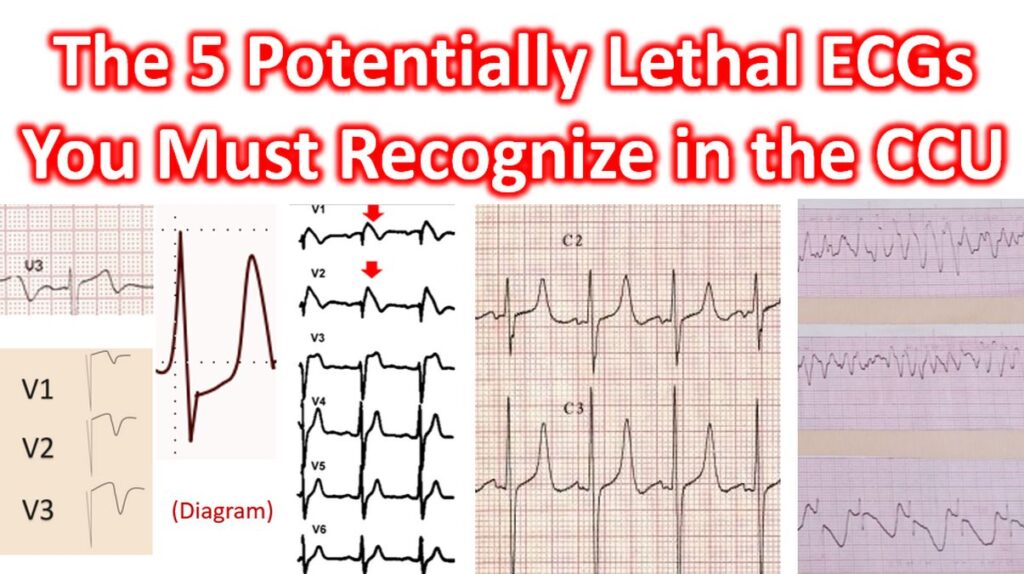
1. Wellens’ Syndrome (Type A & B)
Wellens’ syndrome indicates a critical high-grade stenosis of the proximal Left Anterior Descending (LAD) artery. Patients are often pain-free when the ECG is taken, but they are at imminent risk of a massive anterior wall MI (“The Widowmaker”).
- Pattern: Occurs in the precordial leads (V2–V3).
- Type A: Biphasic T-waves (initial positivity followed by terminal negativity).
- Type B: Deeply and symmetrically inverted T-waves.
- Clinical Pearl: Do not put these patients on a treadmill for a stress test; it can provoke a fatal MI. They need the cath lab.
2. de Winter Syndrome
Considered an STEMI equivalent, this pattern represents acute proximal LAD occlusion but lacks the classic ST-segment elevation.
- Pattern:
- Upsloping ST-segment depression (>1 mm) at the J-point in leads V1–V6.
- Followed by tall, prominent, symmetrical T-waves.
- Often accompanied by 0.5–1 mm ST-elevation in lead aVR.
- Significance: This is an active “evolving” MI that requires primary PCI immediately.
3. Brugada Syndrome
Brugada syndrome is a sodium channelopathy that leads to Ventricular Fibrillation (VF) and sudden cardiac death, often in young, otherwise healthy patients.
- Pattern (Type 1): “Coved” ST-segment elevation >2 mm in >1 right precordial lead (V1–V2), followed by a negative T-wave.
- Clinical Pearl: The pattern can be unmasked by fever, certain medications, or electrolyte imbalances. If you see this in a patient with a history of syncope, it is a high-risk emergency.
4. Hyperkalemia (The “Great Mimicker”)
Severe hyperkalemia (typically K+ > 7.0 mEq/L) can lead to sine-wave patterns and asystole within minutes. It is lethal because it progresses rapidly.
- Progression:
- Peaked T-waves: Narrow-based, “tented” T-waves across all leads.
- P-wave flattening: Leading to the disappearance of P-waves.
- QRS Widening: The QRS begins to merge with the T-wave.
- Sine Wave: The ultimate pre-terminal rhythm.
- Management: Immediate IV Calcium (gluconate or chloride) to stabilize the cardiac membrane.
5. Torsades de Pointes (TdP)
A specific form of polymorphic Ventricular Tachycardia occurring in the context of a prolonged QT interval. It is lethal because it frequently degenerates into Ventricular Fibrillation.
- Pattern: The QRS complexes appear to “twist” around the isoelectric line, constantly changing in amplitude and axis.
- The “R-on-T” Phenomenon: Usually initiated by a PVC falling on the prolonged T-wave of the preceding beat.
- Management: Unlike standard VT, the primary treatment here is Magnesium Sulfate infusion, even if serum magnesium levels are normal. You must also identify and stop any QT-prolonging drugs.