


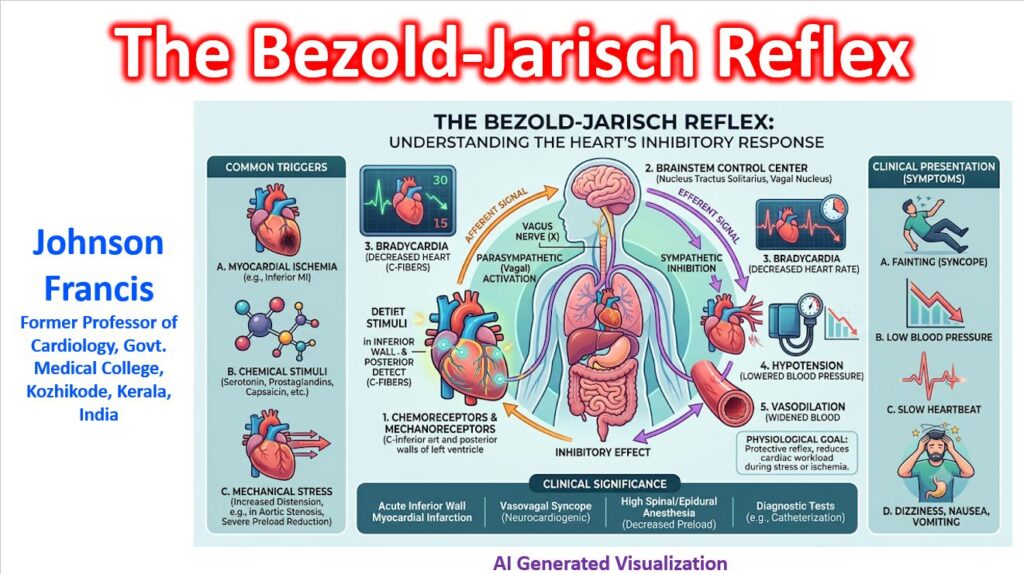

The Bezold-Jarisch reflex (BJR) is an inhibitory cardiovascular reflex originating from receptors within the heart itself. When triggered, it causes a classic triad of bradycardia (slow heart rate), hypotension (low blood pressure), and peripheral vasodilation (widening of blood vessels).
It essentially acts as an emergency “brake” system for the heart. Under normal conditions, a drop in blood pressure triggers the baroreceptor reflex to speed up the heart. The Bezold-Jarisch reflex does the exact opposite, making it a paradoxical and clinically vital phenomenon to understand.
The Reflex Arc: How it Works
The reflex is mediated through an intricate neurochemical pathway:
- Afferent (Input): Non-myelinated C-fibers located primarily in the inferoposterior wall of the left ventricle act as mechanoreceptors and chemoreceptors.
- Triggers: These fibers are stimulated by either mechanical distortion (like a severe lack of volume causing the ventricle to squeeze against itself empty) or chemical triggers (such as ischemia, serotonin, capsaicin, or contrast media).
- Central Processing: The signals travel up the vagus nerve to the nucleus tractus solitarius (NTS) in the brainstem.
- Efferent (Output): The brain responds by massively boosting parasympathetic (vagal) tone to the heart while simultaneously suppressing sympathetic output to the peripheral blood vessels.
Key Clinical Scenarios
In a clinical setting, the Bezold-Jarisch reflex is often the culprit behind sudden, profound bradycardia and drops in blood pressure.
- Inferior Wall Myocardial Infarction (MI): Because the C-fibers are densely concentrated in the inferoposterior wall of the left ventricle, an inferior MI frequently triggers the BJR. Local ischemia and the release of chemical mediators cause sudden bradycardia and hypotension, which can be treated with atropine.
- Severe Hypovolemia & Vasovagal Syncope: When a patient is severely dehydrated or bleeding out, the left ventricle can pump vigorously while empty. This hypercontractile state in a nearly empty chamber mechanically pinches the C-fibers, triggering the BJR. This explains the paradoxical bradycardia seen right before a patient faints from profound hypovolemia or neurocardiogenic syncope.
- Spinal Anesthesia: High spinal anesthesia can cause blood to pool in the lower extremities, severely reducing venous return to the heart. The resulting empty, hypercontractile ventricle triggers the BJR, leading to abrupt bradycardia.
- Aortic Stenosis: Patients with severe aortic stenosis are highly sensitive to sudden changes in afterload and preload, which can mechanically precipitate this reflex.
BJR vs. Other Cardiovascular Reflexes
| Reflex | Primary Trigger | Main Cardiovascular Output |
| Bezold-Jarisch Reflex | Ventricular ischemia, chemical irritants, or severe underfilling | Bradycardia + Hypotension + Vasodilation |
| Baroreceptor Reflex | Changes in arterial stretch/blood pressure | Compensatory (Drops in BP trigger Tachycardia + Vasoconstriction) |
| Bainbridge Reflex | Increased venous return / Right atrial stretch | Tachycardia (To pump out the excess volume) |