



Imagine that you’re in the ER at 0:05. The monitor alarms. You see ST-segment elevation in the precordial leads. Your first instinct? Activate the cath lab. But wait… If you call this a STEMI, you might be sending a patient with Pericarditis for an unnecessary procedure—or worse, missing a life-threatening electrolyte imbalance. Today, we are decoding the Great STEMI Mimics. We’re going beyond pattern recognition to true clinical reasoning.
1. The Big Three: Pericarditis vs. BER vs. STEMI
This is the most common diagnostic dilemma in the ER.
- Acute Pericarditis: * The Look: Diffuse, concave (“smiley face”) ST elevation across almost all leads.
- The Clue: PR-segment depression (especially in Lead II) and PR-elevation in aVR.
- The Ratio: In V6, if the ST-segment height is >25% of the T-wave height, it’s more likely pericarditis.
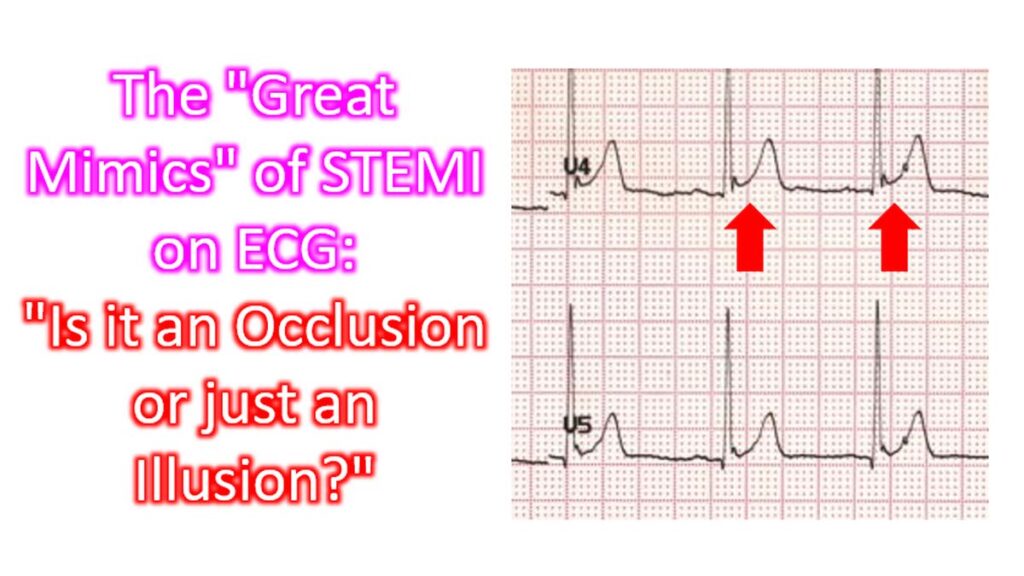
- Benign Early Repolarization (BER): * The Look: High-upward concavity, most prominent in V2–V5.
- The Clue: Look for the “Fishhook” (J-notch) at the end of the QRS complex.
- Stability: Unlike a STEMI, these patterns don’t evolve over minutes or hours.
2. Left Ventricular Hypertrophy (LVH) with “Strain”
LVH often creates deep S-waves in V1–V3 and secondary ST elevation, which can look exactly like an Anteroseptal STEMI.
- How to tell: Look for the Sokolow-Lyon Criteria (S in V1 + R in V5/V6 > 35 mm).
- The Rule of Discordance: In LVH, the ST segment and T-wave should be “discordant” (pointing the opposite way) to the main QRS vector. If the QRS is deeply negative, the ST elevation is expected.
- The Red Flag: If you see concordant ST elevation (QRS and ST segment both pointing up), that’s a real STEMI hiding on top of LVH.
3. Left Bundle Branch Block (LBBB)
A “New LBBB” used to be a STEMI equivalent, but we now know many LBBBs are chronic.
- The Sgarbossa Criteria: This is the “gold standard” in this situation.
- Concordant ST elevation ≥ 1 mm in any lead (Highest specificity).
- Concordant ST depression ≥ 1 mm in V1, V2, or V3.
- Excessive Discordant ST elevation (Modified Smith-Sgarbossa): ST elevation/S-wave ratio > 0.25. That replaces the ≥ 5 mm discordant ST elevation Sgarbossa Criteria.
4. Hyperkalemia (The “Great Mimicker”)
Never forget the metabolic mimics. Potassium shifts can cause “Pseudoinjury” patterns.
- The Look: Widened QRS complexes that “bleed” into the T-wave, creating a sine-wave appearance or peaked T-waves.
- The Danger: If you give thrombolytics to a patient who actually needs calcium gluconate and dialysis, the outcome is disastrous.
Reciprocal Change is the strongest evidence for a STEMI. If you see ST elevation in the Inferior leads (II, III, aVF) AND ST depression in aVL, it is almost certainly a true MI, not a mimic. ST elevation in aVR and possibly V1 is an exception which can occur in pericarditis along with diffuse ST depression in other leads. That is because these leads are oriented to left ventricular cavity.