


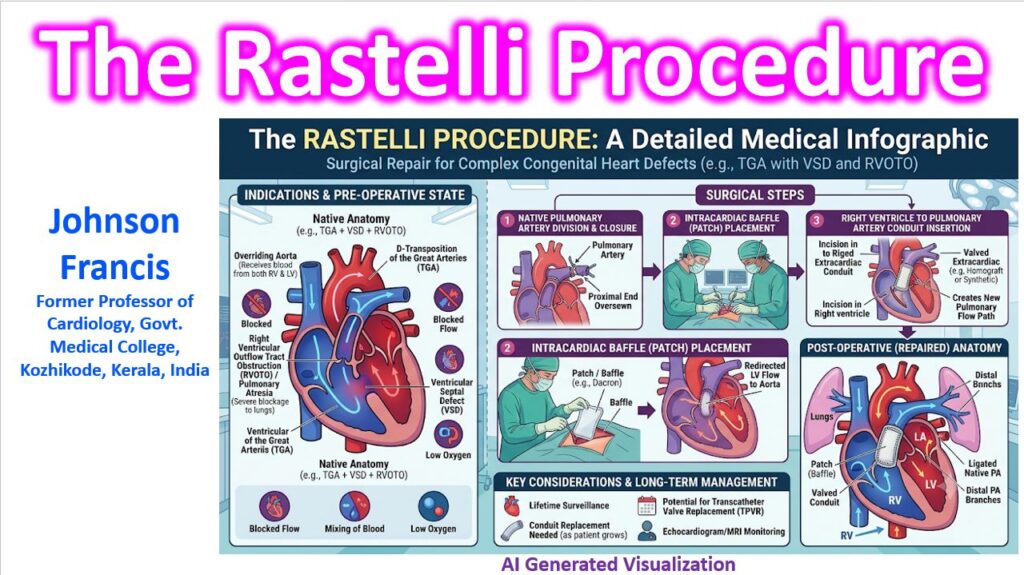

The Rastelli procedure is a definitive surgical repair utilized for complex congenital heart defects characterized by a ventricular septal defect (VSD), an overriding aorta, and severe right ventricular outflow tract obstruction (RVOTO) or pulmonary atresia. Introduced by Rastelli in the late 1960s, it fundamentally re-routes the ventricular hemodynamics to achieve biventricular circulation, bypassing the native, obstructed pulmonary pathway entirely.
Primary Clinical Indications
This approach is most commonly indicated for:
- D-Transposition of the Great Arteries (D-TGA) with a large VSD and left ventricular outflow tract obstruction (LVOTO) / pulmonary stenosis.
- Double Outlet Right Ventricle (DORV), particularly the Fallot-type or those with a subaortic VSD and pulmonary stenosis.
- Tetralogy of Fallot (ToF) with pulmonary atresia or severe anomalous coronary anatomy crossing the RVOT.
- Truncus Arteriosus (often a modified Rastelli approach).
Surgical Mechanics: The “Baffle and Conduit” Approach
The success of the procedure relies on two major structural modifications:
- The Intracardiac Baffle (LV-to-Aorta): The surgeon creates an intracardiac tunnel using a synthetic patch (often Dacron or Gore-Tex). This patch closes the VSD while simultaneously baffling the left ventricular outflow directly into the overriding aorta.
- The Extracardiac Conduit (RV-to-PA): Because the intracardiac baffle often obstructs the native right ventricular outflow tract, and the native pulmonary valve is usually dysplastic or atretic, the native pulmonary artery is permanently ligated or oversewn. A valved conduit (homograft, jugular vein, or synthetic) is then anastomosed from an incision in the anterior wall of the right ventricle to the bifurcation of the pulmonary arteries.
Structural Prerequisites
For a Rastelli to be hemodynamically viable, specific anatomical criteria must be met:
- The VSD must be non-restrictive and located close to the aortic valve (subaortic). If it is restrictive or remote, it must be surgically enlarged, which carries a risk of heart block due to the proximity of the conduction system.
- The left and right ventricles must be of adequate size and function to support systemic and pulmonary circulation, respectively.
Long-Term Management Strategy
When structuring a long-term care plan, the Rastelli procedure is unequivocally a “lifetime management” commitment rather than a permanent cure.
Because the extracardiac conduit is a fixed diameter, it does not grow with a pediatric patient. Furthermore, all biologic and synthetic conduits are subject to structural deterioration, calcification, and pseudointimal peel formation over time. This leads to progressive conduit stenosis, regurgitation, or a combination of both.
Patients require rigorous echocardiographic surveillance to monitor RV pressure and function. Most will require multiple conduit replacements throughout their lives. Today, the timeline for surgical re-intervention can often be extended significantly through Transcatheter Pulmonary Valve Replacement (TPVR), provided the existing conduit provides an adequate landing zone.