



Tricuspid Stenosis (TS) is a valvular heart disease characterized by the narrowing of the tricuspid valve orifice, which creates a mechanical obstruction to blood flow from the right atrium (RA) into the right ventricle (RV) during diastole.
Etiology
While TS is relatively rare compared to left-sided valvular lesions, it typically occurs in conjunction with mitral or aortic valve disease.
- Rheumatic Heart Disease: The most common cause globally. It almost never occurs as an isolated rheumatic lesion and is nearly always associated with mitral stenosis.
- Carcinoid Syndrome: Often leads to fibrous plaque deposition on the endocardial surfaces, resulting in both TS and tricuspid regurgitation (TR).
- Congenital: Tricuspid atresia or congenital webs.
- Other Causes: Infective endocarditis (large vegetations), right atrial myxoma, systemic lupus erythematosus (Libman-Sacks endocarditis), or iatrogenic causes such as pacemaker lead interference. The latter two are unlikely to cause significant tricuspid stenosis. Tricuspid regurgitation is more likely.
Pathophysiology
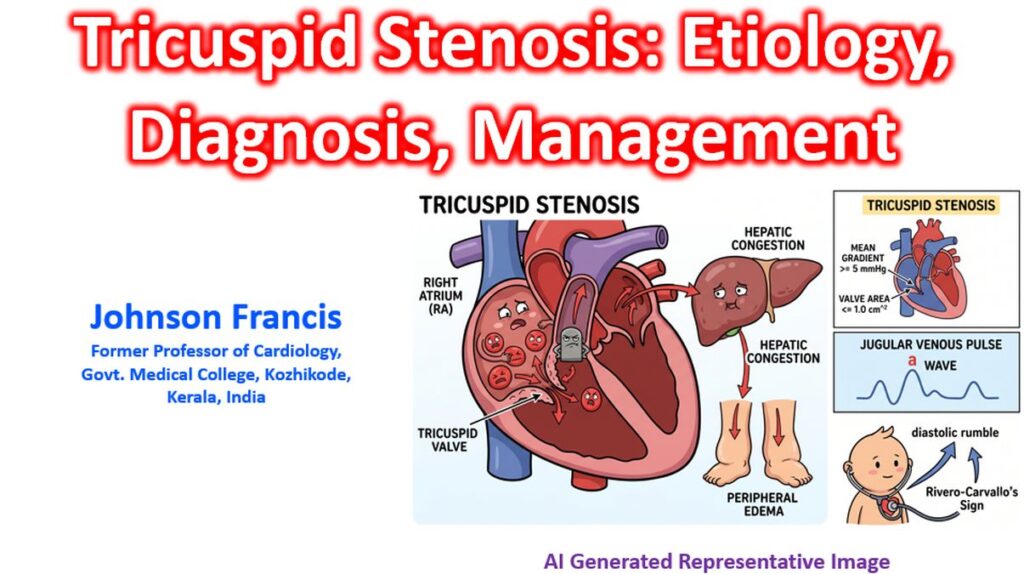
The narrowing results in a pressure gradient between the RA and RV. Unlike the left side, even a small mean pressure gradient (e.g., > 5 mmHg) is considered clinically significant. That is because it is a low pressure system and the tricuspid valve has the largest cross sectional area among the heart valves.
- Systemic Venous Congestion: Elevated RA pressure is transmitted backward into the venae cavae, leading to jugular venous distension, hepatic congestion, and peripheral edema.
- Reduced Cardiac Output: Limited RV filling leads to decreased stroke volume, particularly during exercise.
Clinical Presentation
Symptoms
- Fatigue and Dyspnea: Due to low cardiac output.
- Right-Sided Heart Failure: Abdominal fullness or bloating (ascites), right upper quadrant pain (hepatic congestion), and lower extremity edema.
Physical Examination Findings
- Jugular Venous Pulse (JVP): Characterized by a prominent, flickering “a” wave due to forceful atrial contraction against a stenotic valve.
- Auscultation: A soft, high-pitched diastolic rumble heard best at the lower left sternal border. Unlike the murmur of mitral stenosis, the TS murmur increases in intensity during inspiration (Rivero-Carvallo’s sign).
Diagnostic Evaluation
Echocardiography is the primary tool for diagnosis and severity grading. Key findings include:
- Leaflet Morphology: Thickened, distorted leaflets with restricted motion (doming in diastole).
- Hemodynamics:
- Mean Pressure Gradient: A mean gradient ≥ 5 mmHg at a normal heart rate is generally considered indicative of significant TS.
- Valve Area: A tricuspid valve area (TVA) of ≤ 1.0 cm2 defines severe stenosis.
- Pressure Half-Time: To estimate TVA, is less validated than for mitral stenosis.
Management
Treatment is typically indicated when patients become symptomatic or are undergoing surgery for other valvular lesions.
- Medical Management: Diuretics are the mainstay to reduce systemic venous congestion and alleviate symptoms of edema and ascites.
- Invasive Interventions:
- Percutaneous Balloon Tricuspid Commissurotomy: May be considered in isolated TS without significant TR, though its use is limited compared to mitral valvuloplasty.
- Surgical Repair or Replacement: Usually performed during surgery for left-sided valves. Bioprosthetic valves are often preferred in the tricuspid position due to a lower risk of thrombosis compared to mechanical valves in the low-pressure right heart environment.