



Both Cardiac Resynchronization Therapy (CRT) devices provide biventricular pacing to coordinate the contraction of the right and left ventricles. This corrects mechanical dyssynchrony, improves cardiac output, and reduces heart failure symptoms.
The primary difference lies entirely in the presence or absence of defibrillation capabilities.
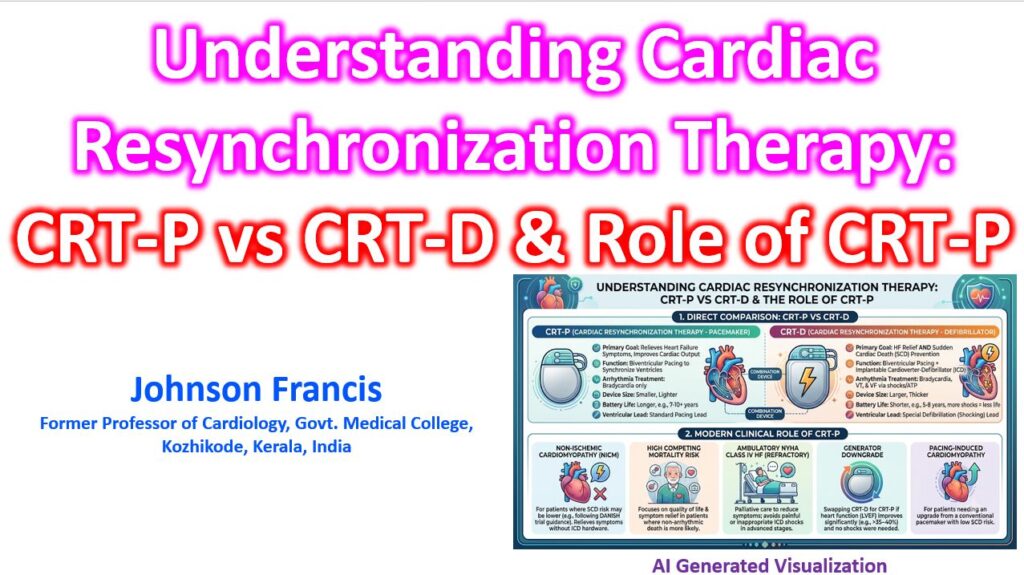
- CRT-P (Pacemaker): Provides resynchronization therapy and pacing for bradycardia. It cannot treat malignant ventricular tachyarrhythmias.
- CRT-D (Defibrillator): Combines biventricular pacing with an implantable cardioverter-defibrillator (ICD). It monitors for ventricular tachycardia (VT) and ventricular fibrillation (VF), delivering anti-tachycardia pacing (ATP) or high-voltage shocks to terminate them.
Clinical Comparison
| Feature | CRT-P | CRT-D |
| Primary Goal | Relieve HF symptoms, reverse remodeling | Symptom relief + Sudden Cardiac Death (SCD) prevention |
| Arrhythmia Treatment | Bradycardia only | Bradycardia, VT, and VF |
| Device Profile | Smaller and thinner | Larger and thicker (houses shock capacitors) |
| Battery Longevity | Typically 7–10+ years | Typically 5–8 years (depletes faster if shocks occur) |
| Ventricular Lead | Standard RV pacing lead | RV defibrillation lead (single or dual coil) |
The Role of CRT-P in Modern Practice
Historically, CRT-D was the default choice for most eligible patients because the criteria for CRT (LVEF ≤ 35%) automatically met the criteria for primary prevention ICD placement. However, the role of CRT-P has expanded significantly based on recent trial data and a better understanding of competing mortality risks.
CRT-P is strongly considered—and often preferred—in the following scenarios:
1. Non-Ischemic Cardiomyopathy (NICM)
The DANISH trial demonstrated that prophylactic ICD implantation does not significantly reduce overall mortality in patients with non-ischemic HFrEF. Consequently, for patients with NICM and a pacing indication (e.g., LBBB, wide QRS), CRT-P provides the symptomatic and remodeling benefits of resynchronization without the added hardware, cost, and complication risks of a defibrillator.
2. High Competing Mortality Risk (Frailty/Comorbidities)
In elderly patients or those with severe comorbidities (advanced CKD, severe COPD, malignancy), the risk of dying from pump failure or non-cardiac causes often outweighs the risk of sudden arrhythmic death. An ICD might successfully terminate an arrhythmia, only for the patient to succumb shortly after to progressive heart failure. CRT-P focuses on quality of life and symptom relief without outliving its benefit.
3. Severe Heart Failure (Ambulatory NYHA Class IV)
For patients with refractory Class IV heart failure who are not candidates for advanced therapies (LVAD or heart transplant), ICD shocks offer no meaningful survival benefit and can cause significant physical and psychological distress. CRT-P is utilized here primarily for palliation and symptom management.
4. Generator Downgrades
When a CRT-D battery depletes, downgrading to a CRT-P generator is a viable strategy for patients who have never received an appropriate shock during the life of the device, particularly if their LVEF has normalized (>35-40%) due to successful resynchronization.
5. Pacing-Induced Cardiomyopathy
Patients who require an upgrade from a conventional dual-chamber pacemaker due to a high right-ventricular pacing burden and subsequent LV dysfunction often only require a CRT-P, provided their baseline risk for SCD remains low.