


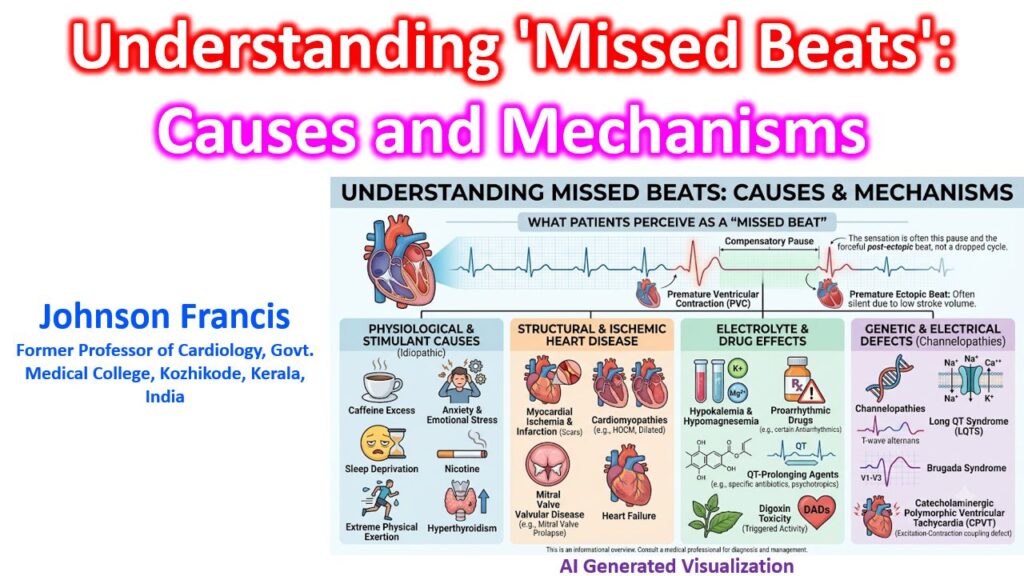

What patients typically perceive as a “missed beat” is rarely an actual dropped electrical cycle (like in a high-degree AV block). Most often, the sensation is the compensatory pause following a premature ectopic contraction—usually a Premature Ventricular Contraction (PVC) or Premature Atrial Contraction (PAC). The premature beat itself usually goes unfelt because its abbreviated diastolic filling time results in a low stroke volume. It is the post-ectopic beat that causes the sensation of a “thud” or “skip.” The prolonged compensatory pause allows for increased ventricular filling, leading to a much more forceful contraction via the Frank-Starling mechanism.
Etiology and Pathophysiology
At a cellular level, these ectopic beats are driven by enhanced automaticity, triggered activity (early or delayed afterdepolarizations), or localized re-entry circuits. These mechanisms can be activated by a variety of clinical and environmental factors:
1. Increased Sympathetic Tone (Benign/Idiopathic)
In structurally normal hearts, ectopy is highly sensitive to catecholamine surges or vagal withdrawal:
- Stimulants: Caffeine, nicotine, cocaine, and amphetamines.
- Physiological Stress: High anxiety, sleep deprivation, or extreme physical exertion.
- Endocrine/Metabolic: Hyperthyroidism and hypoglycemia.
2. Structural and Ischemic Heart Disease
Ectopy in these settings carries a higher clinical weight due to the substrate for sustained arrhythmias:
- Ischemia and Infarction: Myocardial scarring creates heterogeneous conduction velocities, forming the perfect anatomical substrate for re-entry circuits. Acute ischemia also alters resting membrane potentials, causing early afterdepolarizations (EADs).
- Heart Failure and Cardiomyopathies: Elevated ventricular end-diastolic pressure and direct myocardial stretch alter the electrophysiological properties of myocytes. This is a common mechanism in Hypertrophic Obstructive Cardiomyopathy (HOCM), Dilated Cardiomyopathy, and Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC).
- Valvular Disease: Mitral valve prolapse (MVP) and severe aortic stenosis induce mechanical stretch and secondary electrical instability in the myocardium.
3. Electrolyte Derangements
Alterations in intra- and extracellular ion gradients heavily influence the action potential duration:
- Hypokalemia and Hypomagnesemia: Prolong the repolarization phase (Phase 3), significantly increasing the risk of EADs and frequent PVCs.
- Hypercalcemia: Shortens the QT interval and can increase overall ventricular irritability.
4. Proarrhythmic Drug Effects
- Antiarrhythmics: Paradoxically, Class IA, IC, and III agents can lengthen the QT interval or slow conduction enough to promote re-entry.
- Digoxin Toxicity: Inhibits the Na+/K+ ATPase pump, increasing intracellular calcium. This leads to delayed afterdepolarizations (DADs) and classic presentations like ventricular bigeminy.
- QT-Prolonging Agents: Macrolides, fluoroquinolones, and various psychotropic medications.
5. Channelopathies
Genetic defects in myocardial ion channels can predispose patients to frequent ectopy and potentially lethal arrhythmias, even in the absence of structural disease:
- Long QT Syndrome (LQTS): Driven by EAD-mediated ectopy.
- Brugada Syndrome: Caused by epicardial dispersion of repolarization, primarily in the right ventricle.
- Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT): Ryanodine receptor mutations cause a massive calcium leak and subsequent DADs during exercise or emotional stress.