



Both septal bounce and septal shudder are hallmark echocardiographic findings of constrictive pericarditis (CP). While they look slightly different on an echo, they are driven by the exact same hemodynamic mechanism: enhanced ventricular interdependence within a fixed total cardiac volume. Because a scarred, rigid pericardium prevents normal free-wall expansion during diastole, the heart operates in a fixed space. Any change in filling volume in one ventricle must happen at the direct, immediate expense of the other.
Septal Bounce (The “Shift”)
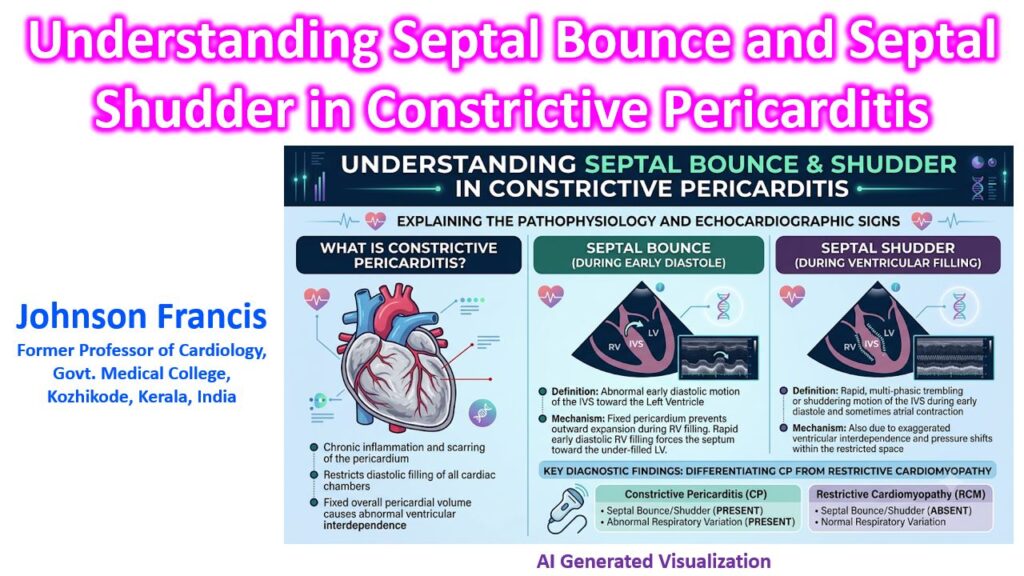
The septal bounce is a macroscopic, early diastolic shift of the interventricular septum (IVS) toward the left ventricle (LV).
- Mechanism: During inspiration, negative intrathoracic pressure increases venous return to the right ventricle (RV). Since the RV free wall cannot expand outward against the constricting pericardium, the rapid early diastolic filling physically forces the septum to bow leftward into the LV to accommodate the volume.
- Echo Appearance: On M-mode or 2D imaging (parasternal short or long axis), you will see an abrupt leftward motion of the IVS during early diastole, which then “bounces” back to a more central position as filling pressures equilibrate later in diastole.
Septal Shudder (The “Vibration”)
While related to the bounce, a septal shudder is a high-frequency, rapid, multi-phasic trembling of the IVS.
- Mechanism: This typically occurs during isovolumic relaxation time (IVRT) or immediately following atrial contraction. Because the pericardial space is fixed, the instantaneous pressure gradients between the RV and LV during these transient phases create a brief “tug-of-war.” The septum acts as a flexible membrane vibrating rapidly between two rigid, pressure-locked chambers as valves open and close.
- Echo Appearance: On M-mode, it presents as a transient shivering or “notching” of the septal line right as the ventricles transition into diastole, often occurring just before the more pronounced macroscopic bounce.
The Clinical Differentiator
When evaluating a patient with heart failure and preserved ejection fraction, differentiating CP from restrictive cardiomyopathy (RCM) is notoriously difficult. RCM lacks both the shudder and the bounce because the pericardium remains compliant, meaning the ventricles do not share the exaggerated interdependence seen in CP.