



The Prothrombin Time (PT) and International Normalized Ratio (INR) are fundamental assays for evaluating the extrinsic and common pathways of the coagulation cascade. While the test is a routine part of clinical practice, breaking down the nuances of these metrics can be incredibly valuable for patient education. Here is a breakdown of the clinical mechanics, target ranges, and practical pearls for managing patients on Vitamin K Antagonists (VKAs) like warfarin.
The Mechanics: PT vs. INR
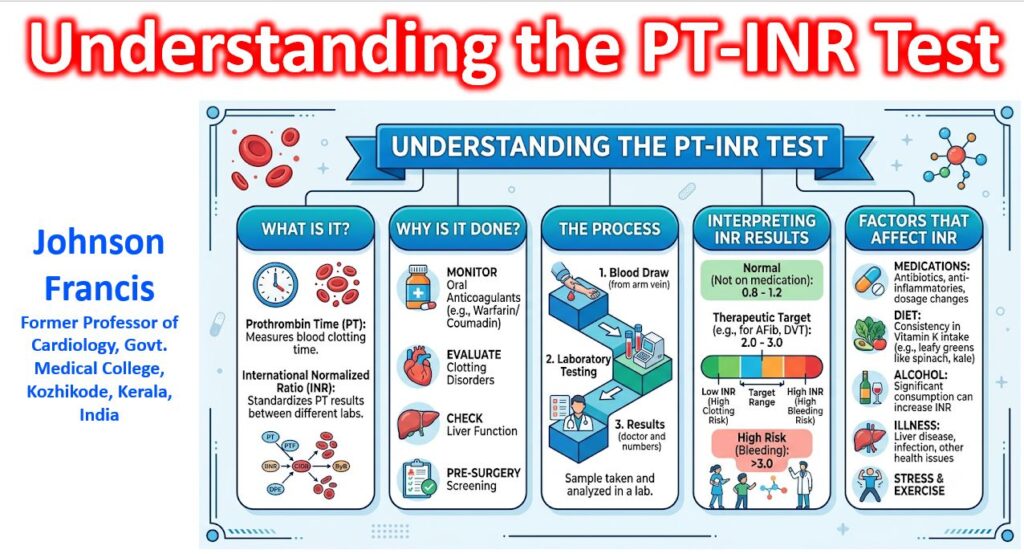
Prothrombin Time (PT) measures the time (in seconds) it takes for plasma to clot after the addition of tissue factor (thromboplastin) and calcium. It specifically assesses the function of factors VII, X, V, II (prothrombin), and I (fibrinogen).
Because different labs use different tissue factor formulations, a patient’s PT can vary wildly from one lab to another. The INR was developed to standardize these results. It is calculated using the International Sensitivity Index (ISI) of the specific thromboplastin reagent used:
INR = [(PTpatient)/(PTnormal)]ISI
Target Therapeutic Ranges
For a healthy individual not on anticoagulation therapy, a normal INR is approximately 1.0 (range 0.8–1.1). When patients are on VKAs, the target shifts based on their thromboembolic risk:
| Indication | Target INR Range |
| DVT / PE (Treatment & Prophylaxis) | 2.0 – 3.0 |
| Non-valvular Atrial Fibrillation | 2.0 – 3.0 |
| Aortic Mechanical Valve (Bileaflet/Current Gen) | 2.0 – 3.0 |
| Mitral Mechanical Valve | 2.5 – 3.5 |
| Mechanical Valve + AFib or Hypercoagulable State | 2.5 – 3.5 |
Key insight: The newer generation of mechanical valves (like the On-X aortic valve) has changed the landscape slightly, with the FDA approving a lower target INR of 1.5 – 2.0 (plus low-dose aspirin) after the first three months, significantly reducing bleeding risks while maintaining efficacy.
Clinical Pearls for Management
Managing a patient’s INR requires navigating a minefield of drug-drug and drug-food interactions.
1. Dietary Vitamin K Consistency
VKAs work by inhibiting the enzyme vitamin K epoxide reductase (VKORC1). Patients often mistakenly believe they need to completely avoid Vitamin K. The actual goal is consistency. Sudden spikes or drops in Vitamin K intake will destabilize the INR.
When advising patients on their diet, it is highly effective to use local, culturally relevant examples. For instance, highlighting the high Vitamin K content in regional staples like red amaranth, drumstick leaves (moringa), or heavy coconut-based curries with leafy greens helps patients visualize their daily intake much better than generic lists of “kale and spinach.”
2. The Antibiotic and Amiodarone Spikes
The hepatic cytochrome P450 system (specifically CYP2C9) metabolizes warfarin. Two common clinical scenarios that cause dangerous INR spikes:
- Amiodarone: Initiating amiodarone for rhythm control will significantly inhibit warfarin metabolism. A pre-emptive 30-50% reduction in the warfarin dose is often required.
- Antibiotics: Broad-spectrum antibiotics (like fluoroquinolones or trimethoprim/sulfamethoxazole) not only interact with CYP enzymes but also eradicate the gut flora responsible for synthesizing endogenous Vitamin K, leading to a rapid rise in INR.
3. Point-of-Care (POC) Testing vs. Venipuncture
POC coagulometers are fantastic for home monitoring or quick clinic checks, relying on capillary whole blood. However, they can lose accuracy at higher INR values (typically > 4.5). If a POC device reads unusually high, a traditional venipuncture lab draw is mandatory to confirm before administering Vitamin K or Four-Factor Prothrombin Complex Concentrate (4F-PCC).