


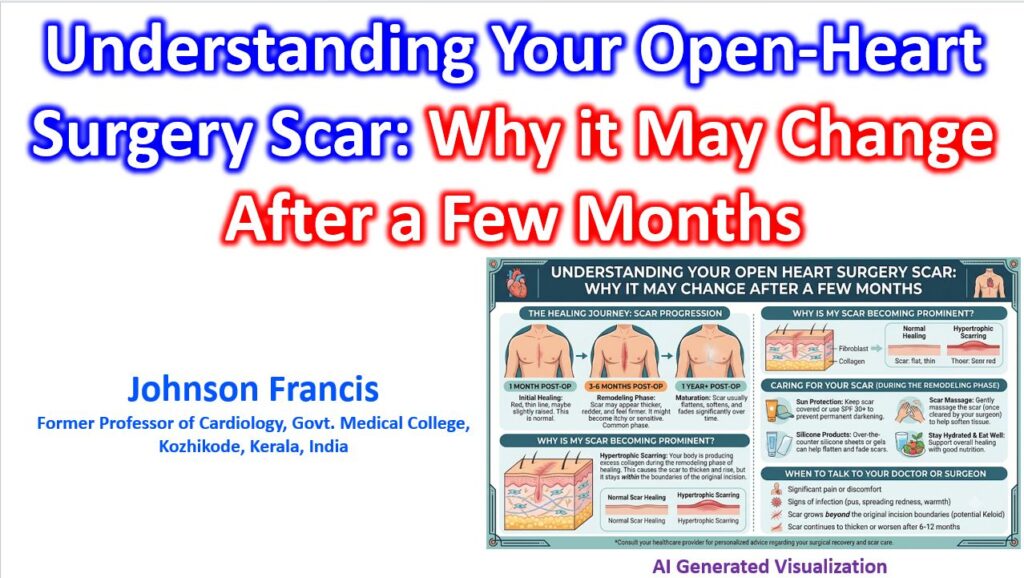

The presternal region is notoriously prone to aberrant scar remodeling following a median sternotomy. It is a common clinical trajectory for a wound to appear well-approximated and flat in the immediate postoperative period, only to become increasingly raised, erythematous, and pruritic between the 2- and 6-month mark. This typically occurs because the wound is transitioning from the proliferative phase to the remodeling phase under constant mechanical stress.
Pathophysiology of Sternal Scarring
The sternum is subject to continuous cyclical tension from respiration, coughing, and pectoral muscle movement. Mechanotransduction pathways convert this physical stress into chemical signals, predominantly upregulating TGF-β expression.
This leads to a prolonged inflammatory response and an overactive fibroblast profile. The normal remodeling process—where immature Type III collagen is gradually replaced by a highly organized matrix of Type I collagen—is disrupted. The result is a disorganized, nodular overproduction of collagen and delayed apoptosis of myofibroblasts.
Clinical Differentiation
When evaluating a prominent post-sternotomy scar, the primary distinction is between a hypertrophic scar and a keloid, as this dictates the management strategy.
| Feature | Hypertrophic Scar | Keloid |
| Boundaries | Confined to original incision margins | Extends beyond original wound margins |
| Timeline | Develops within 1-6 months | Can develop months to years later |
| Trajectory | May spontaneously regress over 1-2 years | Rarely regresses; continuous growth |
| Vascularity | Highly vascular (erythematous) | Less dense neovascularization |
Therapeutic Modalities
Early intervention during the active remodeling phase yields the best functional and cosmetic outcomes.
- Silicone Gel Sheeting: Gel sheets are soft and self-adhesive. The first-line prophylactic and therapeutic option. It hydrates the stratum corneum, which downregulates fibroblast proliferation and reduces capillary hyperemia. To be effective, sheets must be worn for 12–24 hours daily.
- Intralesional Corticosteroids: Triamcinolone acetonide (TAC) injections suppress VEGF, inhibit fibroblast growth, and promote collagen degradation. These are highly effective for reducing bulk and pruritus but carry a risk of local atrophy and telangiectasia.
- Intralesional 5-Fluorouracil (5-FU): Often used in combination with TAC for recalcitrant scars, 5-FU inhibits pyrimidine synthesis, inducing fibroblast apoptosis.
- Pulsed Dye Laser (PDL): Highly effective for the erythematous phase. The 585-595 nm wavelength targets oxyhemoglobin, destroying the microvasculature feeding the hyperactive scar tissue, thereby inducing localized ischemia and reducing the scar’s bulk.