



Congenital Mitral Stenosis is a rare, complex cardiac anomaly characterized by an anatomical obstruction of the left ventricular inflow. Unlike the acquired version often seen in adults with rheumatic heart disease, congenital mitral stenosis is defined by a primary developmental failure of the mitral valve apparatus.
## Pathological Types
Congenital mitral stenosis was divided into four types by Ruckman & Van Praagh (1978, cited in)
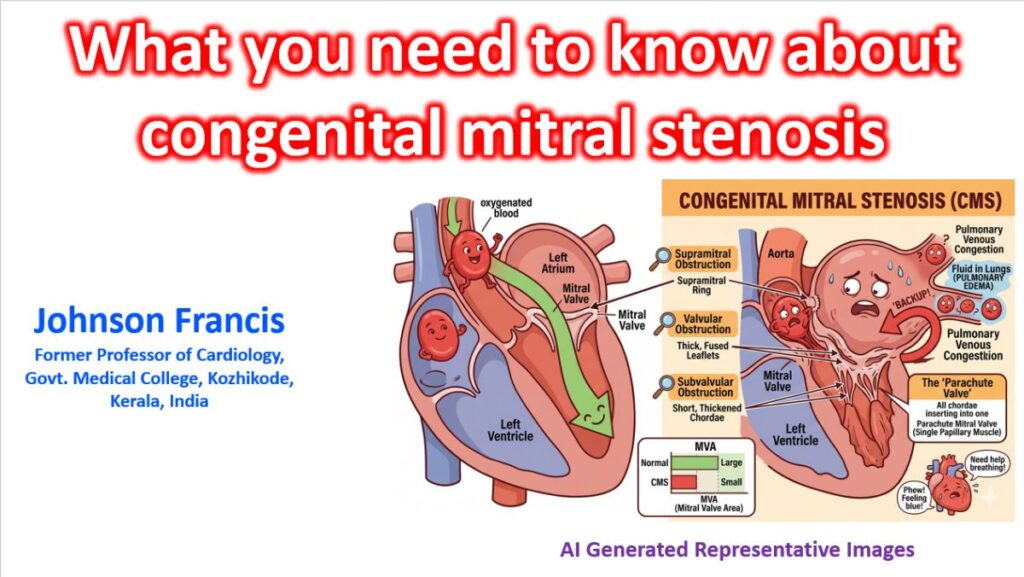
- Typical Congenital Mitral Stenosis: Characterized by thickened leaflets and shortened, fused chordae with narrow interchordal spaces. This is the most common variety.
- Hypoplastic Mitral Stenosis: A miniature version of a normal valve, typically seen in Hypoplastic Left Heart Syndrome (HLHS). Second most common variety. Noted in infancy and has never been reported as a de novo diagnosis in adults.
- Supramitral Ring: A fibrous diaphragm just above the mitral annulus (a classic part of Shone complex). Some consider this to be an acquired lesion resulting from turbulent flow across the mitral valve.
- Parachute Mitral Valve: All chordae tendineae insert into a single, dominant papillary muscle. Though this is the least common form of congenital mitral stenosis, it is discovered the most frequently as a de novo diagnosis in the adult population.
## Shone Complex
CMS is frequently a component of Shone Complex, a series of obstructive lesions on the left side of the heart.
- Supramitral ring.
- Parachute mitral valve.
- Subaortic stenosis.
- Coarctation of the aorta.
## Clinical Presentation
The severity of symptoms depends on the degree of obstruction and the presence of associated shunts (like an ASD, which can “decompress” the left atrium).
- Symptoms: Tachypnea, poor feeding, failure to thrive, and recurrent pulmonary infections (due to pulmonary venous congestion).
- Physical Exam: * Loud S1 and an apical mid-diastolic rumble.
- Unlike rheumatic MS, an opening snap is usually absent because the leaflets are thick and non-pliable rather than fused at the tips.
- Signs of right ventricular hypertrophy (RV heave) if pulmonary hypertension has developed.
## Diagnostic Evaluation
### Echocardiography (Gold Standard)
Assessment focuses on the Simpson’s Biplane method for volumes and specific Doppler hemodynamics:
- Mean Pressure Gradient: Elevated gradients (often > 5-10 mmHg) indicate significant stenosis.
- Pressure Half-Time (T1/2): Used to calculate the Mitral Valve Area (MVA), though less reliable in infants with high heart rates.
- Morphology: Identification of “parachute” deformity or supramitral rings.
### Cardiac Catheterization
Reserved for cases where non-invasive imaging is inconclusive or to precisely measure Pulmonary Capillary Wedge Pressure (PCWP) and pulmonary vascular resistance prior to surgery.
## Management Strategies
### Medical Management
Primarily supportive to manage pulmonary congestion:
- Diuretics: To reduce preload and pulmonary edema.
- Afterload reduction: Generally avoided as it may compromise systemic perfusion in the setting of fixed inflow obstruction.
### Surgical Intervention
Surgery is challenging due to the small size of the valve and the risk of inducing mitral regurgitation.
- Mitral Valvuloplasty: Commissurotomy or resection of accessory chordae/supramitral rings.
- Valve Replacement: Used only as a last resort in infants. The small “annulus-to-patient” ratio often leads to patient-prosthesis mismatch. Mechanical valves are preferred over bioprosthetic ones due to durability, but they require lifelong anticoagulation.
## Prognosis
The outlook is generally guarded and depends heavily on the presence of other left-sided obstructions. Patients require lifelong follow-up with a pediatric or adult congenital cardiologist to monitor for restenosis and the development of pulmonary hypertension.