



Monophasic defibrillators have been almost entirely phased out of clinical practice because biphasic waveforms achieve higher first-shock success rates using significantly less energy, directly reducing post-resuscitation myocardial injury. The ultimate goal of defibrillation is delivering sufficient current to the myocardium to depolarize a critical mass of tissue without causing electroporation or stunning. Monophasic technology struggled to optimize this balance, particularly in challenging patients.
The Limitations of Monophasic Waveforms
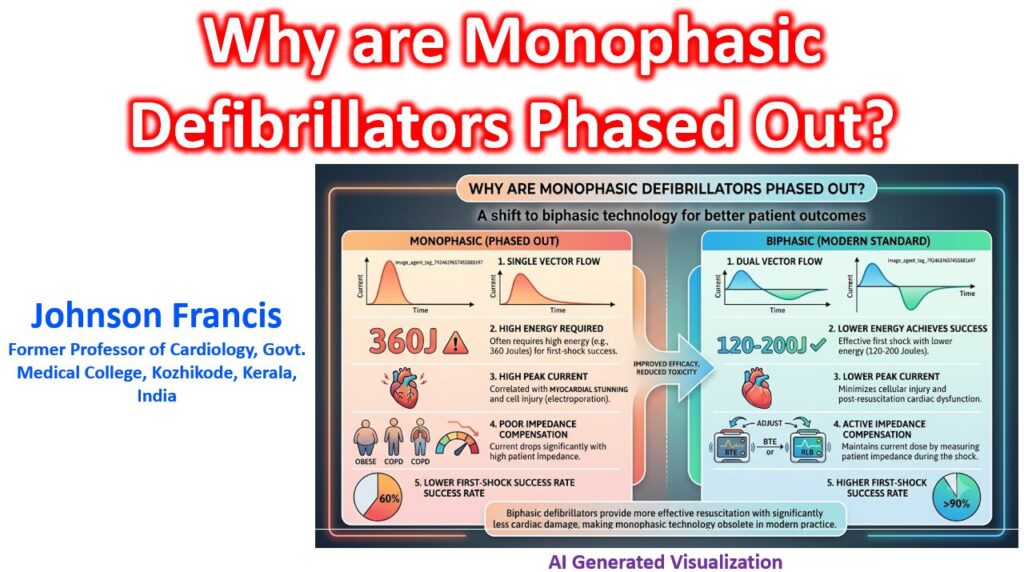
Monophasic defibrillators delivered current in a single vector from one pad to the other, typically using a damped sine or truncated exponential waveform at 360 Joules. This “brute force” approach had two major clinical flaws:
- High Peak Current and Myocardial Stunning: To ensure enough current reached the heart to terminate ventricular fibrillation (VF), the initial peak current had to be extremely high. This high peak current is directly correlated with myocardial injury, leading to post-shock AV block, ST-segment changes, and reduced left ventricular ejection fraction (myocardial stunning) in the immediate post-resuscitation phase.
- Vulnerability to Patient Impedance: Monophasic devices lacked active mechanisms to compensate for transthoracic impedance (TTI). In a high-impedance patient—due to body habitus, severe COPD, or poor pad contact—the actual current delivered to the myocardium dropped precipitously, leading to a much higher rate of shock failure.
The Biphasic Advantage
Biphasic waveforms reverse the polarity of the current partway through the shock. This fundamental change solved the monophasic limitations through two mechanisms:
Lower Defibrillation Thresholds
By reversing the current flow, biphasic shocks essentially “sweep” the myocardium in two directions. The first phase depolarizes a large portion of the myocardium, and the reverse phase lowers the defibrillation threshold of the remaining cells. This permits the successful termination of VF/VT at much lower energy levels (typically 120-200J). The reduced peak current significantly minimizes cellular electroporation and subsequent post-shock myocardial dysfunction.
Active Impedance Compensation
Modern biphasic devices measure the patient’s transthoracic impedance between the pads during the shock and dynamically adjust the waveform parameters to ensure the correct dose of current is delivered:
- Biphasic Truncated Exponential (BTE): The device lengthens the duration of the shock in high-impedance patients to ensure the necessary area-under-the-curve (current over time) is maintained.
- Rectilinear Biphasic (RLB): The device dynamically alters the voltage to maintain a constant current delivery across the first phase, regardless of patient impedance.
Key Insight: The superiority of biphasic waveforms is clearest in real-world clinical data: biphasic shocks demonstrate a first-shock success rate for VF exceeding 90%, compared to roughly 60% for 360J monophasic shocks.