What are ventricular ectopic beats (VPC)?
What are ventricular ectopic beats (VPC)?
Ventricular ectopic beats are premature heart beats originating from the ventricles, the lower chambers of the heart. Normal heart beats originate from the sinus node, situated in the right upper chamber. Sinus node is the natural pacemaker of the heart which gives out regular electrical pulses to induce contractions of the heart. Ventricular ectopic beats (VEB) are also known by other names like ventricular premature complex (VPC), premature ventricular complex (PVC) and ventricular premature beat (VPB). Ventricular ectopic is the commonest heart rhythm abnormality.
In a ventricular ectopic beat, the sequence of activation of the heart is different from that in the normal sinus beat. Normal sinus beat activates the upper chambers first and then the lower chambers, after a short delay. Upper chambers are the right and left atrium. Lower chambers are the right and left ventricle. The delay is produced by a second relay station known as the atrioventricular (AV) node, situated at the junction between the upper and lower chambers, in the lower part of right atrium.
The delay between the activation of the upper and lower chambers ensure that the contraction of the upper chambers is over before the lower chambers start contracting. This ensures that the lower chambers get a booster filling effect when the upper chambers contract (atrial help). Rest of the filling of the ventricles occur passively when they relax after a contraction. In ventricular ectopic beats, this sequence is lost.
Ventricles contract first when the signals arise from the lower chambers in ventricular ectopic beat. The signals may be conducted back to the upper chambers which contract after the lower chambers. So the ventricles do not get help in filling from the atria. Moreover, as the contraction of the ventricles occur earlier than normally, they do not get enough time to fill. Poorly filled ventricle is not able to eject much blood so that the volume of the pulse is low or even absent.
When the upper chambers contract soon after the lower chambers, the blood from the upper chambers cannot enter the lower chambers as the valves between them are closed. This results in back flow of blood into the veins which return deoxygenated blood into the heart. This back flow may be felt as a pulsation in the neck.
If the number of ventricular ectopics is more than 10% of the total heart beats, it can produce weakening of heart muscle function gradually. The abnormal sequence of activation produces dyssynchrony in the left ventricle and some of them can go in for left ventricular failure in the long run. But if the frequency of ventricular ectopics is low, it hardly affects the function of the heart. Ventricular ectopics may be there in many near normal individuals.
Though isolated ventricular ectopic beats are of no great significance, sometimes they can be the fore runner of more serious heart rhythm disorders. Ventricular ectopy in general indicates an irritable ventricle. This can sometimes lead to continuous firing of the abnormal focus, leading to ventricular tachycardia. Ventricular tachycardia is an abnormal fast rhythm originating from the lower chambers of the heart. It is a potentially serious condition.
Occasionally a very premature ventricular ectopic beat can also lead to a lethal heart rhythm abnormality known as ventricular fibrillation. Ventricular fibrillation produces stoppage of the heart and is fatal unless immediate cardiopulmonary resuscitation (CPR) and defibrillation (electrical countershock) are delivered by a trained or semi-trained person. This is more likely to occur in those with other structural heart disease like a heart attack.
Ventricular ectopics can occur without significant other heart disease and it is the usual pattern. Abnormalities in the blood electrolytes like a low potassium or magnesium level can increase the irritability of the heart and lead to ectopic beats. A structurally abnormal heart is more prone for VPC. Failure due to any cause like heart attack, heart muscle disease and heart valve disease can increase the chance of VPC. Risk of progression to ventricular tachycardia or ventricular fibrillation is higher if there is other associated heart disease.
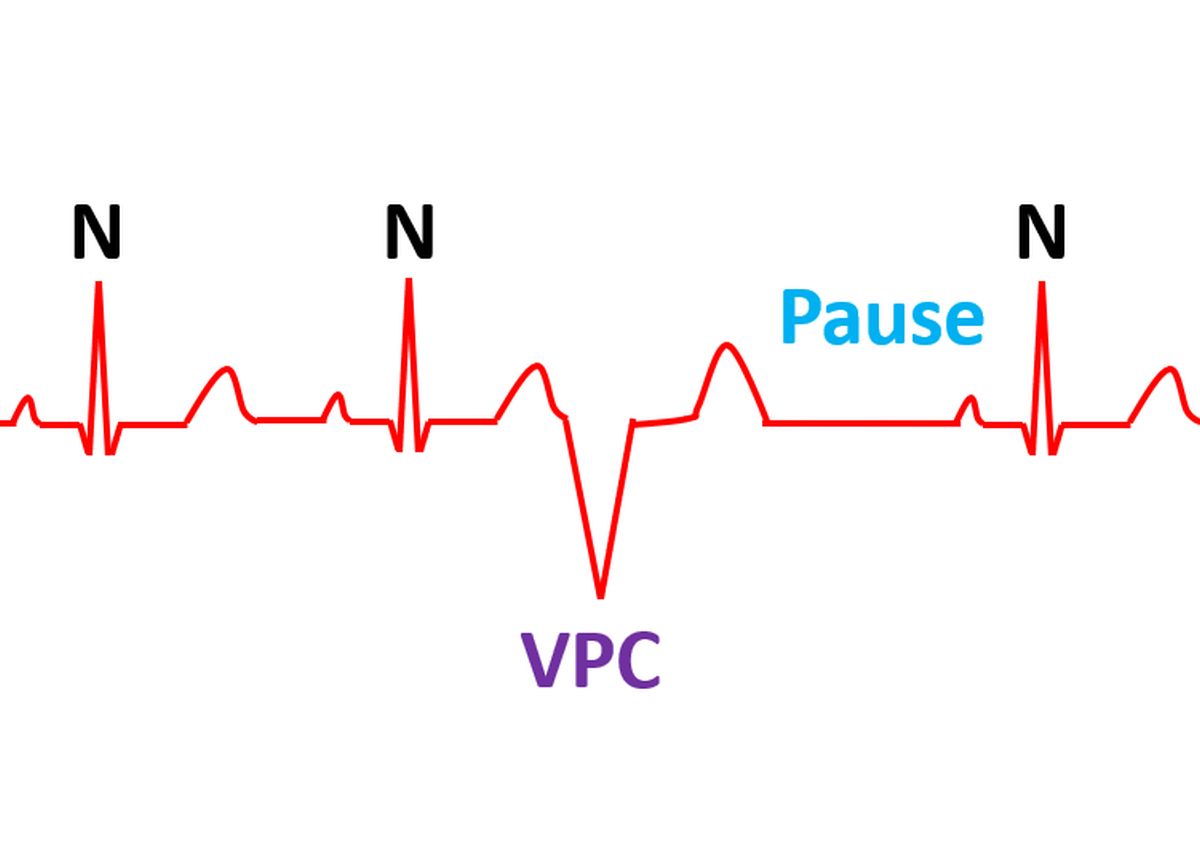
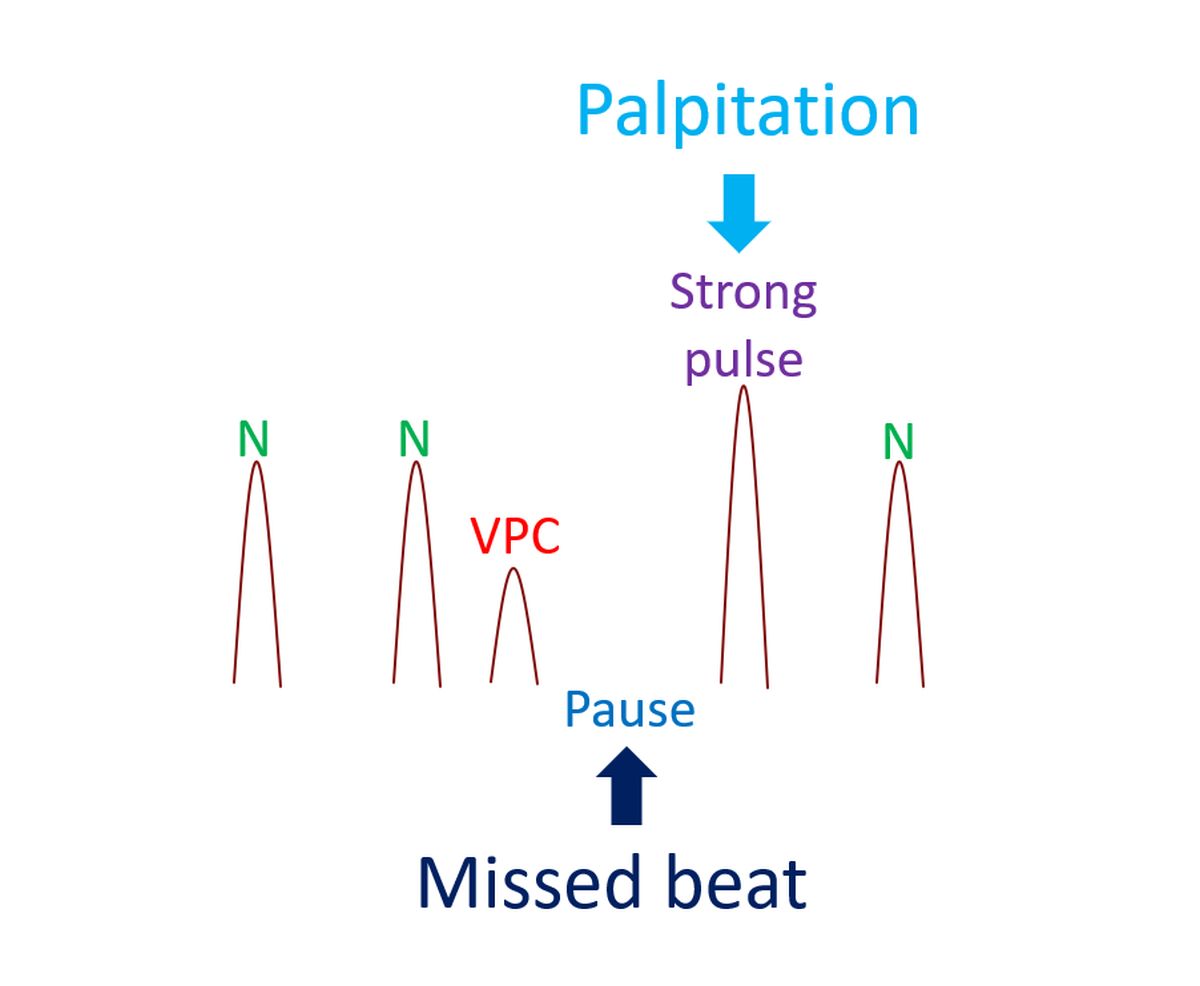
Ventricular ectopics are often appreciated as missed beats while feeling the pulse. This is because the poorly filled ventricles produce a weak pulse. The beat after that is stronger as it gets more time to fill after a short pause which is usual after a VPC. This forceful contraction is often felt by the individual and causes palpitation.
Some individuals get higher frequency of VPC on taking caffeinated drinks. Hence it is better to avoid them. ECG (electrical recording of the heart) is a simple test which can document a PVC. They stand out as broad premature complexes in the ECG, followed by a pause and can be easily recognized by even a minimally trained person. The total number of PVC in a day can be documented by an ambulatory Holter monitor. Holter monitor is a continuous ECG recorder attached to the belt and connected to the chest with lead wires.
If there is an associated structural heart disease or heart failure, it needs immediate attention and can reduce the number of PVCs. Abnormalities of blood potassium and magnesium levels have to be corrected. Occasionally there may be some medications taken by the person which has induced the VPCs. Stopping them can also reduce the number of ventricular ectopics.
Medications to suppress ventricular ectopics are available, but are not generally preferred if the PVCs are isolated and not associated with structural heart disease or heart failure. This is because of potential long term adverse effects of some of these medications. They may be given if essential, as decided by the physician, with monitoring for adverse effects.
Very rarely, large number of VPCs can produce heart failure and need extra treatment. In selected cases, an electrophysiology study (EP study) is done to find out the exact location of the abnormal focus. This is done by introducing small wires into the heart under local anaesthesia and recording the electrical signals from various parts of the heart. If a significant abnormality is found, it can be treated by catheter ablation. In catheter ablation, the tiny region producing the abnormality is inactivated by a radiofrequency signal delivered at the exact spot.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal