What is a perimembranous VSD?
What is a perimembranous VSD?
Perimembranous VSD is the commonest type of VSD. VSD stands for ventricular septal defect, a hole in the wall between the lower chambers of the heart. When there is a ventricular septal defect, blood shunts from the left ventricle to the right ventricle. Left ventricle is the lower left chamber and right ventricle the lower right chamber. This leads to increased blood flow to the lungs. VSD usually occurs as a birth defect, though it can rarely occur in the adult after a heart attack. If the VSD is very large, excessive blood flow to the lungs, which returns to the left ventricle later can sometimes lead to heart failure.
Important locations of VSD are perimembranous, muscular, outlet and inlet. Outlet VSD is near the outlet of the ventricles, near the origin of the great arteries. The great artery arising from the right ventricle is the pulmonary artery, which takes blood to the lungs for oxygenation. Aorta is the great artery arising from the left ventricle, which carries oxygenated blood to the whole body. Perimembranous VSD is in the upper part of the interventricular septum, where it is thin and like a membrane. Interventricular septum is the technical name for the wall between the two lower chambers. Muscular VSD is a defect in the thick muscular part of the interventricular septum.
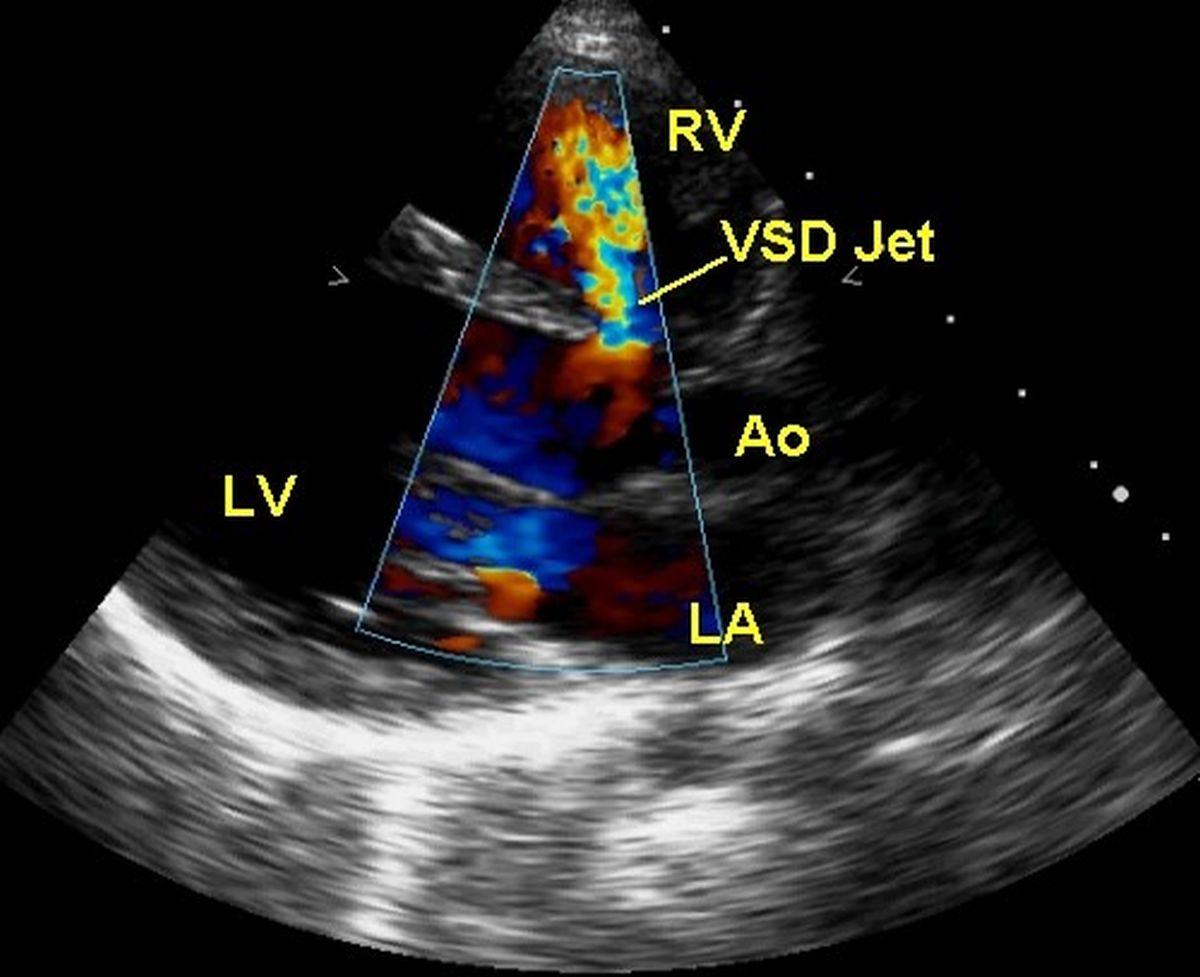
Perimembranous VSD can be suspected clinically when there is a heart murmur heard over the left side of the chest, near the midline. In small VSD, it is often a loud murmur due to the turbulent flow across the defect. Murmur is softer in large VSD because the pressure gradient between the two ventricles will be low. Presence of the large defect equalizes the pressures in the two chambers. It is a systolic murmur, meaning that it is heard when the heart contracts. Perimembranous VSD can be documented by an ultrasound study of the heart known as echocardiogram, as shown here.
When a perimembranous VSD is detected in a baby, there is a chance that it can close spontaneously over a period of time. Chance for spontaneous closure is more for a small VSD than a large VSD. Even large VSD can decrease in size gradually. If a large VSD decreases in size later, it may even be left alone and followed up with certain precautions like prompt treatment of all infections. Lifetime risk of a small VSD is the occasional occurrence of an infection in that region, which can be dangerous. But it is very rare with meticulous treatment of all infections. Perimembranous VSD which remains large may have to be closed by surgery, early in life . Device closure for perimembranous VSD without surgery is evolving and is not as popular as device closure of muscular VSD. Device closure is done by introducing special folded devices through tiny holes made in the blood vessel of the groin, under continuous X-ray imaging.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal