What is mitral stenosis?
What is mitral stenosis?
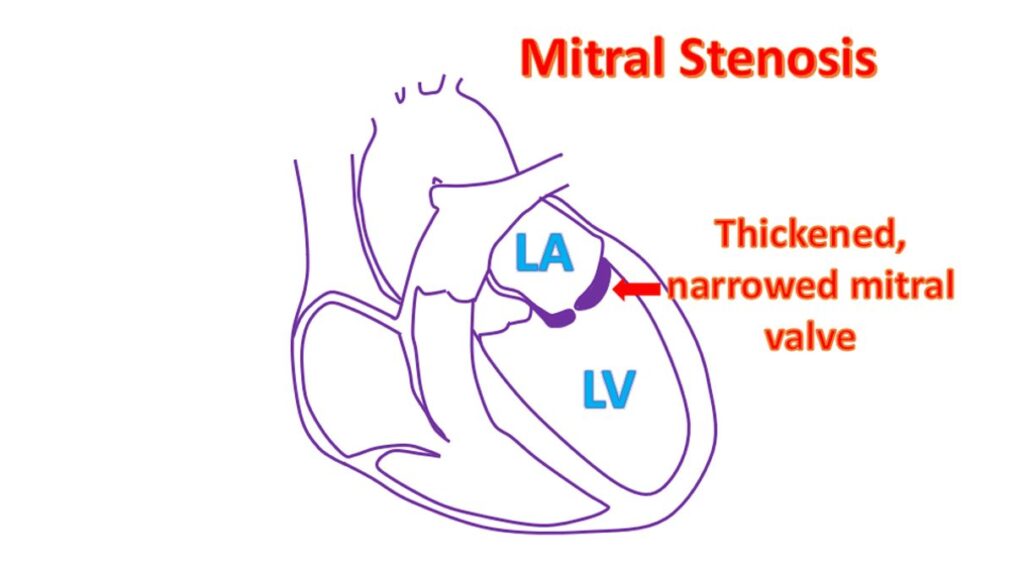
Mitral stenosis is narrowing of the valve between the left atrium and left ventricle. Left atrium is the left upper chamber which receives oxygenated blood from the lungs. Left ventricle is the lower muscular chamber of the heart which pumps oxygenated blood to the whole body. Mitral stenosis is usually a sequelae of rheumatic fever, a disease which affects the major joints and heart valves. Another form of mitral stenosis is due to calcification of the mitral valve base, seen in elderly.
Mitral stenosis is a progressive disease, with the obstruction progressing gradually. It can occur in young age in developing countries and is then known as juvenile mitral stenosis, typically before the age of 20 years. It can also be adult onset and late onset, depending on the time at which symptoms start. Juvenile mitral stenosis usually progresses more rapidly than the other varieties and is thought to be due to recurrent episodes of rheumatic fever.
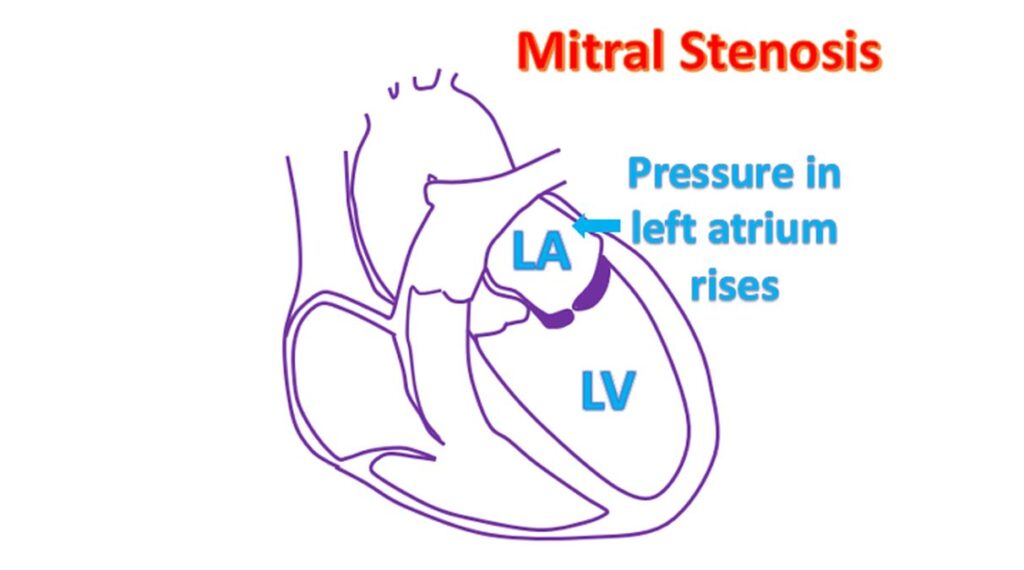
Obstruction to the blood flow from the left atrium to the left ventricle leads to damming up of blood in the left atrium. Left atrial pressure rises and is transmitted back to the pulmonary veins which carry oxygenated blood from the lungs.
When the pressure in the lungs go high, typically above 25 mm Hg, fluid starts collecting in the tiny air spaces of the lungs known as alveoli. This impairs oxygen exchange in the lungs and oxygen saturation in the blood falls. This condition is known as pulmonary edema. As the lungs are heavier, breathing becomes progressively more difficult.
Persons with severe mitral stenosis may wake up at night suddenly with breathlessness, which is relieved after sitting up for some time. This is technically called paroxysmal nocturnal dyspnea and is a characteristic feature often noted in mitral stenosis. Sometimes the small blood vessels of the lungs may break due to the high pressure causing bleeding into the lungs and spitting out blood.
When the left upper chamber enlarges due to the pressure load and increased blood volume within it, an irregular fast heart rhythm known as atrial fibrillation can occur. The fast rhythm may be felt as palpitation. This fast rhythm may precipitate heart failure as the blood flow across the narrowed mitral valve becomes poorer in a fast rhythm. Blood clots can form in the left atrium due to stasis of blood. The clots can move into the circulation and get lodged elsewhere.
If it gets lodged in a blood vessel of the brain and blocks it, a portion of the brain gets damaged. This usually results in stroke, causing weakness of one side of the body or a part of it. Persons with mitral stenosis and atrial fibrillation are routinely given medications to prevent clot formation to avoid this. When such medications are given, the clotting function of the blood is monitored regularly using a test known as prothrombin time with international normalized ratio (INR) estimation. This is needed to optimize the dosage of the medication.
Other medications given when there is atrial fibrillation are those which can slow the heart rate and make it regular. This will help to improve the flow of blood across the narrowed valve, though it will not reduce the obstruction. Another medication routinely given for those with rheumatic mitral stenosis is penicillin to prevent recurrence of rheumatic fever. Those allergic to penicillin will receive alternate antibiotics.
Presence of mitral stenosis can be detected by listening to the heart using a stethoscope. When the blood flows to the left ventricle when the heart relaxes after a contraction, a murmur is heard in this phase (mid diastolic murmur). Being a localised murmur, it requires careful listening to pick up. It may not be audible in cases known as silent mitral stenosis.
Usual tests in suspected cases of mitral stenosis are ECG, X-ray of chest and an echocardiogram (ultrasound study of the heart). Echocardiogram can give an estimate of the mitral valve area and hence the severity of stenosis. It can also tell if the valve has a leak in addition. Other valves, functions of heart chambers and pressure in the right ventricle and pulmonary artery (blood vessel of the lungs) can all be assessed by echocardiography.
When the mitral stenosis is very severe, it can be opened up using a balloon attached to a tube, introduced through a small hole in the groin. This procedure is known as balloon mitral valvotomy. If the valve has a lot of calcium deposits, this procedure cannot be done and then open surgical mitral valvotomy can be done.
When the mitral valve has a significant leak in addition to the narrowing, balloon valvotomy is not preferred. The procedure done then is a surgery known as mitral valve replacement. Replacement can be done using mechanical valve or a bioprosthetic valve. Biological valves need medications to prevent clot formation only for a short period. As mechanical valves have a high tendency for clot formation within them, medication to prevent clot formation has to be given lifelong. This requires regular monitoring of blood clotting function with INR estimation as mentioned earlier.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal