What is a wearable cardioverter defibrillator (WCD)?
What is a wearable cardioverter defibrillator (WCD)?
എന്താണ് ധരിക്കാവുന്ന കാർഡിയോവർട്ടർ ഡിഫിബ്രിലേറ്റർ (WCD)?
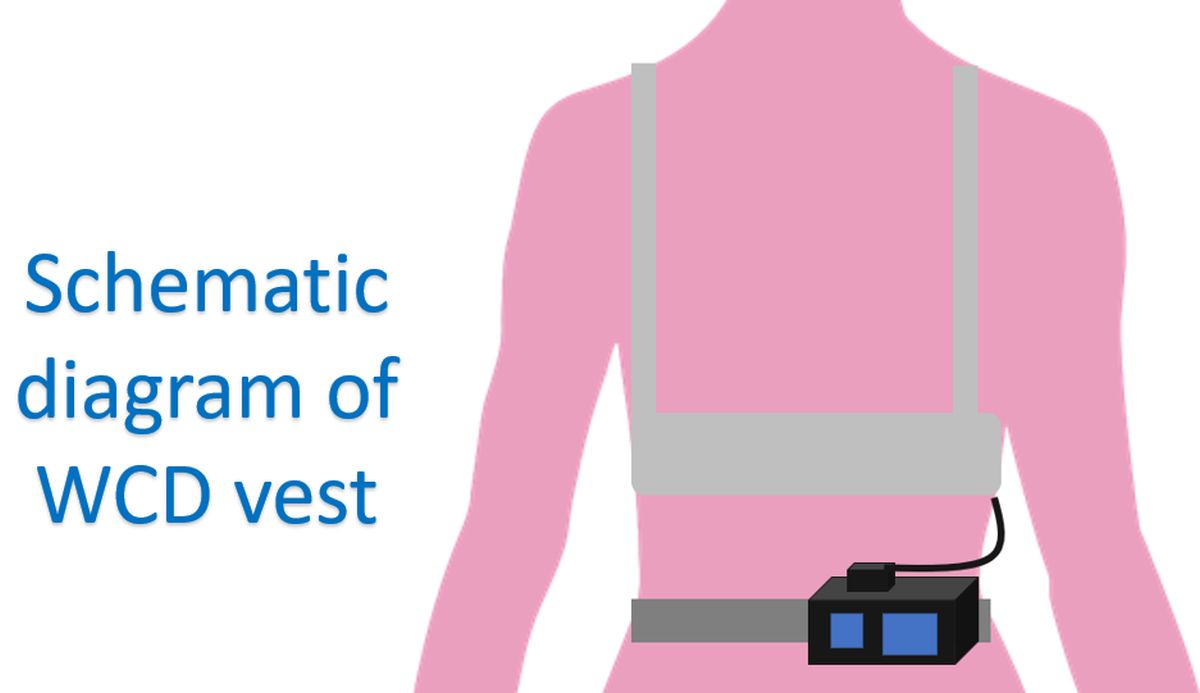
Wearable cardioverter defibrillator (WCD) is a device which is worn on a vest, monitors the heart rhythm continuously and gives a controlled electrical shock in case of life threatening heart rhythm disorders. Implantable cardioverter defibrillator (ICD) is a similar device which is implanted under the skin for long term use. WCD is meant for temporary use for those who have a high risk of life threatening heart rhythm disorders, but are ineligible for an ICD. WCD has patch electrodes for giving the shocks and a monitoring system built-in into a vest while the defibrillator with battery is worn on the belt. WCD can also give audible alerts and does not need the help of a bystander as it works automatically.
A typical WCD device has a maximum shock output of 150 Joules and could terminate the most dangerous heart rhythm abnormalities in first attempt with 70 to 100 Joules shock. Still programming at maximum energy output has been suggested for ambulatory patients to ensure good safety margin. WCD has been called as a “Life vest till the life boat arrives”, meaning that it can be considered during the period when the patient is not eligible for an ICD as per guidelines published by medical societies. These include patients within 40 days of a heart attack who are at high risk of life threatening heart rhythm abnormalities, but still ineligible for ICD as benefits have not been proven. Another, possibly more important reason to use WCD is when an ICD has to explanted due to infection and there is a waiting period before a new one can be implanted.
As expected, the most important “Achilles heel” of a WCD is compliance. Real world studies have shown average daily usage as low as 17.3 hours, which means that there would be no protection during the remaining period! In a randomized controlled trial involving 2302 patients, of the 48 participants who died, only 12 were wearing the device at the time of death. Another compilation of multiple studies with data on over 32,000 patients showed that mortality while wearing WCD is rare, 0.7 per 100 persons over 3 months. Like ICDs, WCD can also give inappropriate shocks sometimes, at a rate of 2 per 100 persons over 3 months. This is due to errors in “judgment” by the automatic monitoring software, by which non-life-threatening fast rates are considered as life-threatening and shocks delivered. Errors can be reduced to some extent by meticulous usage technique and programming of the device.
Studies have shown that compliance is more in those who already had a cardiac arrest during previous hospital admission for heart attack as well as in those who had previous heart failure and more WCD alarms. Poor compliance was noted in those who had any WCD shock. When used during the waiting period after ICD explantation for a new ICD implantation, WCD is thought to be a cost effective option. Usual care typically involves hospital admission for about 21 days while waiting for the new ICD implant till the infection in the previous one has cleared. With the temporary protection given by WCD, if they can go home rather safely and total hospitalization period brought down to about 15 days, a cost saving of 1782 Euros has been estimated.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal