What is ECMO?
What is ECMO?
ECMO stands for extracorporeal membrane oxygenation. ECMO can temporarily support the function of heart and lungs when they are damaged by a reversible disease. It is similar to heart lung machine in function but can be used at the bedside of the patient in the intensive care unit. Heart lung machines are used in open heart surgery theatres to support heart and lung function during major heart operations. Two important components of ECMO are a pump replacing the function of the heart and an oxygenator replacing the function of the lungs. While heart lung machines are used for a relatively short period of a few minutes or hours, ECMO can be used for days, weeks or even more with extreme care. This allows the damaged heart and lungs to recover from the illness which has caused the damage.
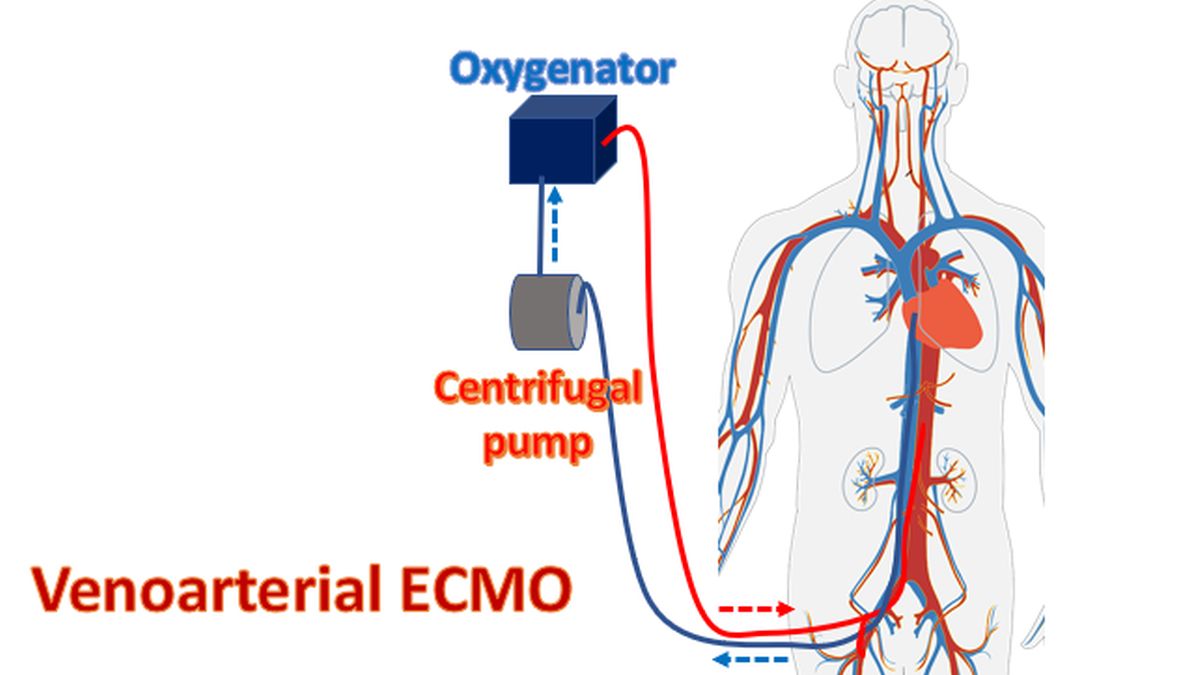
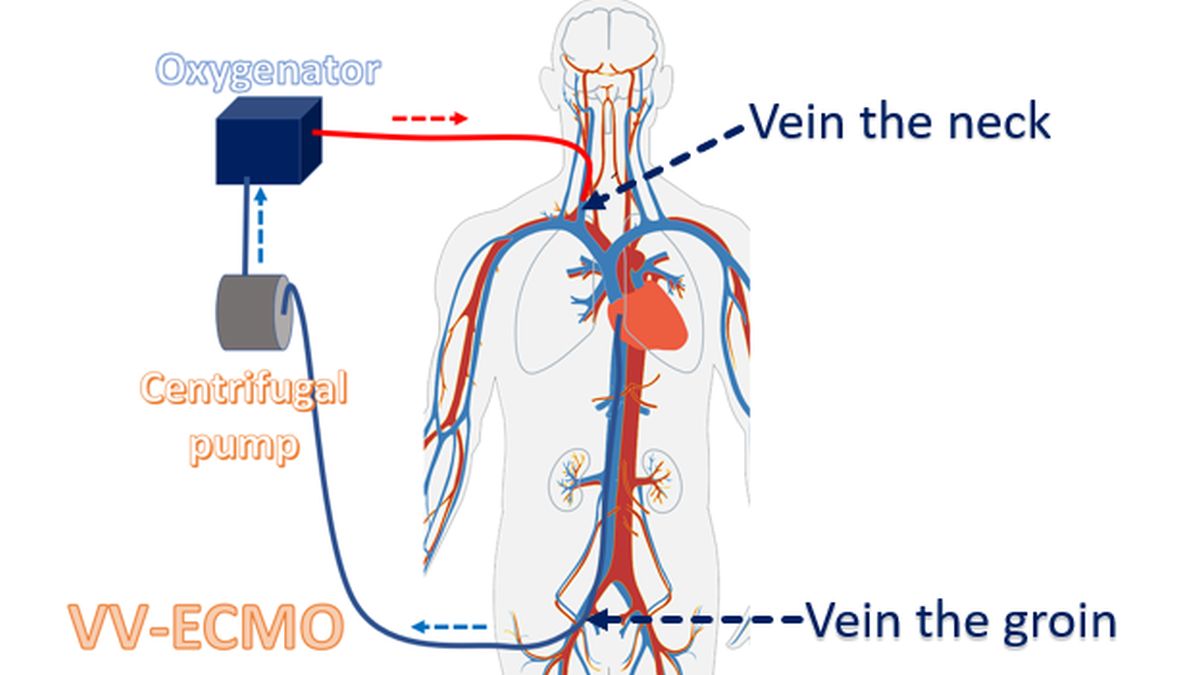
There are two types of ECMO circuits known as veno-arterial (VA-ECMO) and veno-venous (VV-ECMO). VA-ECMO can support the function of both heart and lungs while VV-ECMO is meant to support only lung function, when the heart is functioning well. VA-ECMO takes blood from a vein and delivers it into an artery after oxygenation. Artery is a blood vessel to which heart pumps blood and vein is a blood vessel which passively returns the blood to the heart. In VV-ECMO, blood is taken from one vein and delivered to another vein.
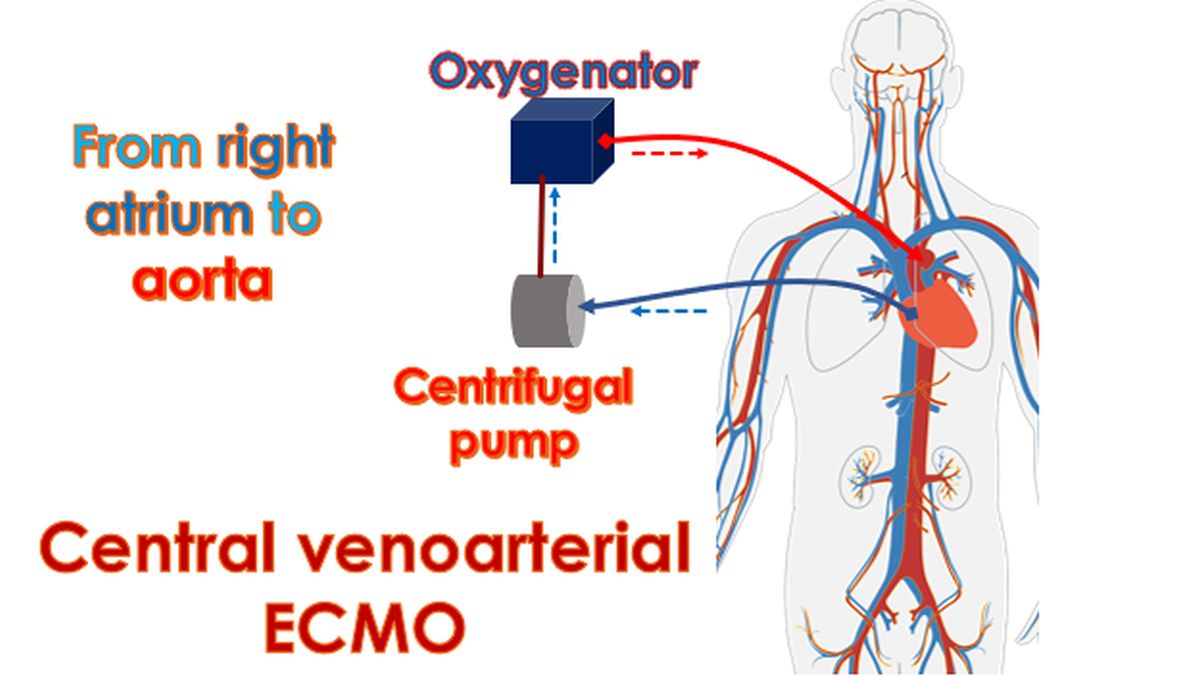
When blood is taken from the right upper chamber of the heart (right atrium) and delivered to the aorta it is called central VA-ECMO. Aorta is the major blood vessel supplying oxygenated blood to the whole body. Central VA-ECMO is done when the chest is already opened and set up for the use of a heart lung machine during surgery. Peripheral VA-ECMO takes blood from the vein in the groin and returns oxygenated blood to the artery in the groin. Relatively large tubes are inserted by operation into the blood vessels for instituting peripheral VA-ECMO.
Extracorporeal Life Support Organization (ELSO) keeps track of ECMO utilization worldwide. In a report published in 2012, 51,000 individuals had received ECMO. Half of them were small babies who had lung failure and overall survival was 75%. Among the 13,000 patients who were treated for supporting the heart, 40-50% survived. By 2016, 78,397 patients had received ECMO, with 58% overall survival. Dashboard on ELSO website shows total of 174,797 cases of which 2,490 belong to this year till date. Total survival is shown as 54%. For heart disease, ECMO is recommended for those with very low blood pressure following a heart attack, not responding to medications. Currently ECMO is an expensive treatment option available only in very few advanced centers.
Potential complications of ECMO include bleeding, clot formation in the ECMO circuit and blood vessels, difficulty in accessing blood vessels for inserting the tubes and infections. Complication rates are higher if the person has already been on breathing machine (ventilator) for a long period and has damage to multiple organs like liver and kidneys in addition. Clot formation can be prevented to some extend by using medications, but that carries a risk of bleeding. Infections can be prevented by meticulous care of the ECMO circuit. In spite of these ECMO is a potentially life saving option for many persons with severe reversible damage to heart and lungs. If the damage is irreversible, they will need heart-lung transplantation to wean off ECMO.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal