What is rupture of sinus of Valsalva aneurysm (RSOV)?
What is rupture of sinus of Valsalva aneurysm (RSOV)?
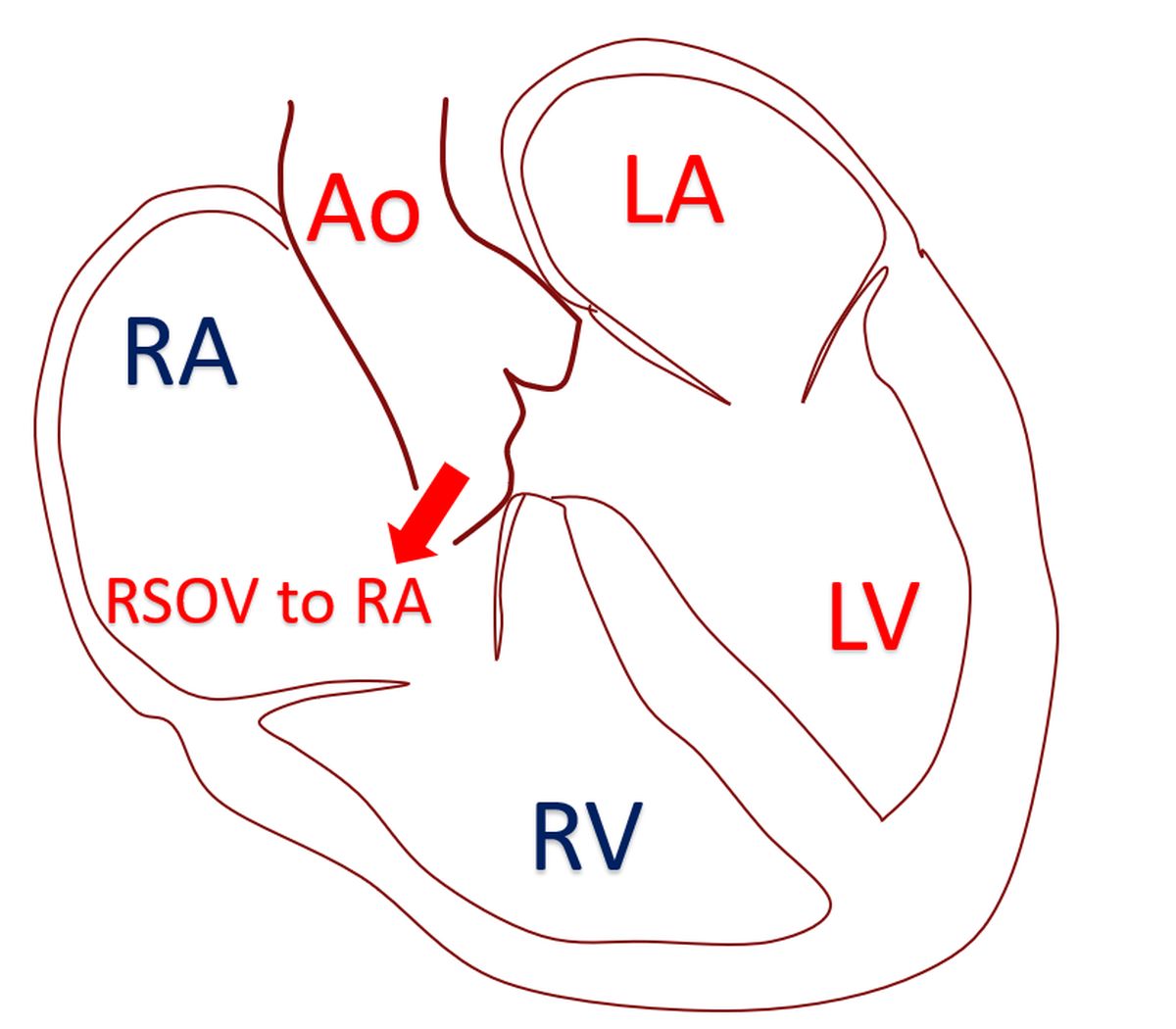
Sinus of Valsalva aneurysm is an enlargement in the root of aorta. Aorta is the largest blood vessel carrying oxygenated blood to the whole body. The aneurysm is usually due to a defect in the wall of the root of aorta, occurring as a birth defect. The aneurysm may compress a nearby heart chamber, blood vessel of the heart or the electrical conduction system of the heart. This can reduce the blood supply to the heart muscle or produce electrical conduction defects. About one third of sinus of Valsalva aneurysms can rupture and produce severe symptoms in about a quarter. Important symptoms after rupture are breathlessness, chest pain and fatigue. Eventually they can go into heart failure.
Rupture of sinus of Valsalva aneurysm (RSOV) usually occurs into the right heart chambers. Rarely rupture can occur into left heart chambers, pericardium, pulmonary artery or superior vena cava. Pericardium is the outer covering of the heart, having two layers. Bleeding into these layers can cause compression of the heart and impede its proper filling, in a condition known as cardiac tamponade, which is a dire emergency. Pulmonary artery is the blood vessel taking blood to the lungs for oxygenation. Superior vena cava is the large blood vessel which returns blood from the upper part of the body into the heart.
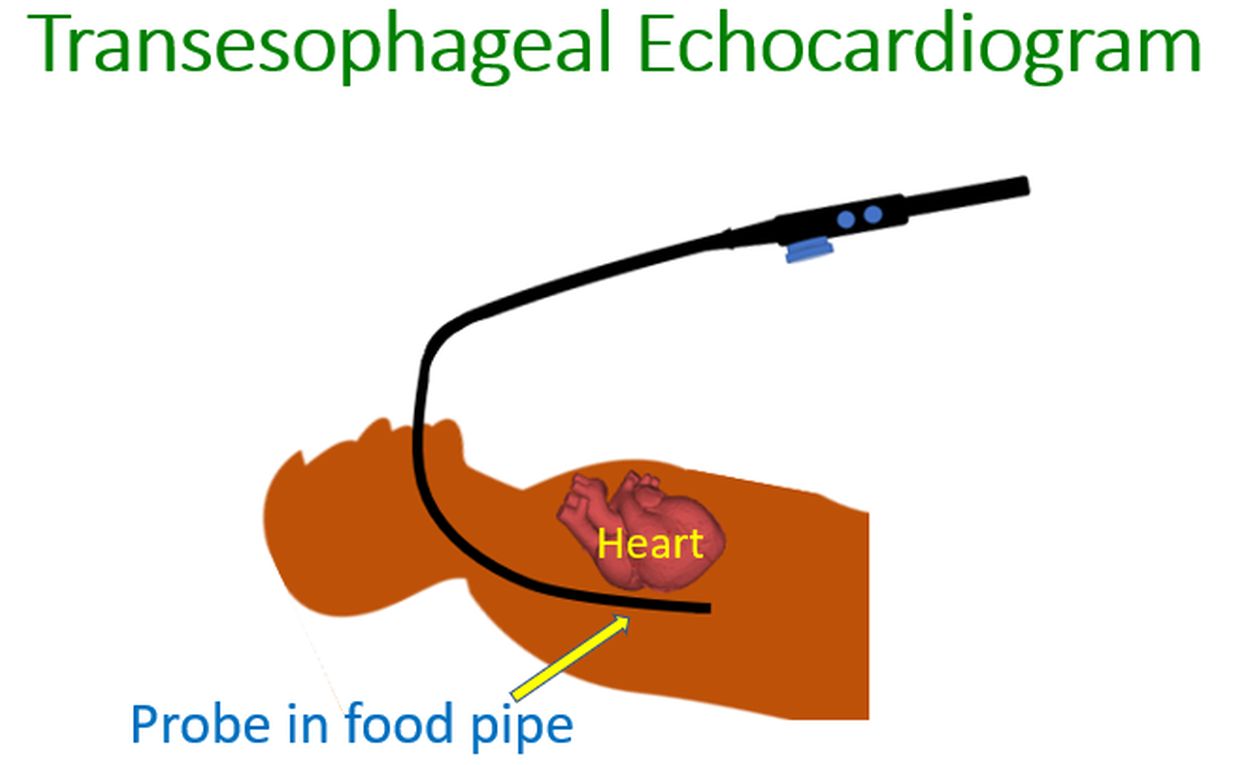
RSOV can be diagnosed by an echocardiogram, the ultrasound study of the heart. Better imaging is obtained by a special echocardiogram known as transesophageal echocardiogram. In transesophageal echocardiogram, the ultrasound probe is introduced into the food pipe which is just behind the heart and gives images with more finer details. Magnetic resonance imaging (MRI) and computed tomography (CT scan) are other useful tests in a case of RSOV. X-ray imaging of the blood vessels of the heart after injecting radiocontrast medication, known as coronary angiography, may be done in preparation for surgery.
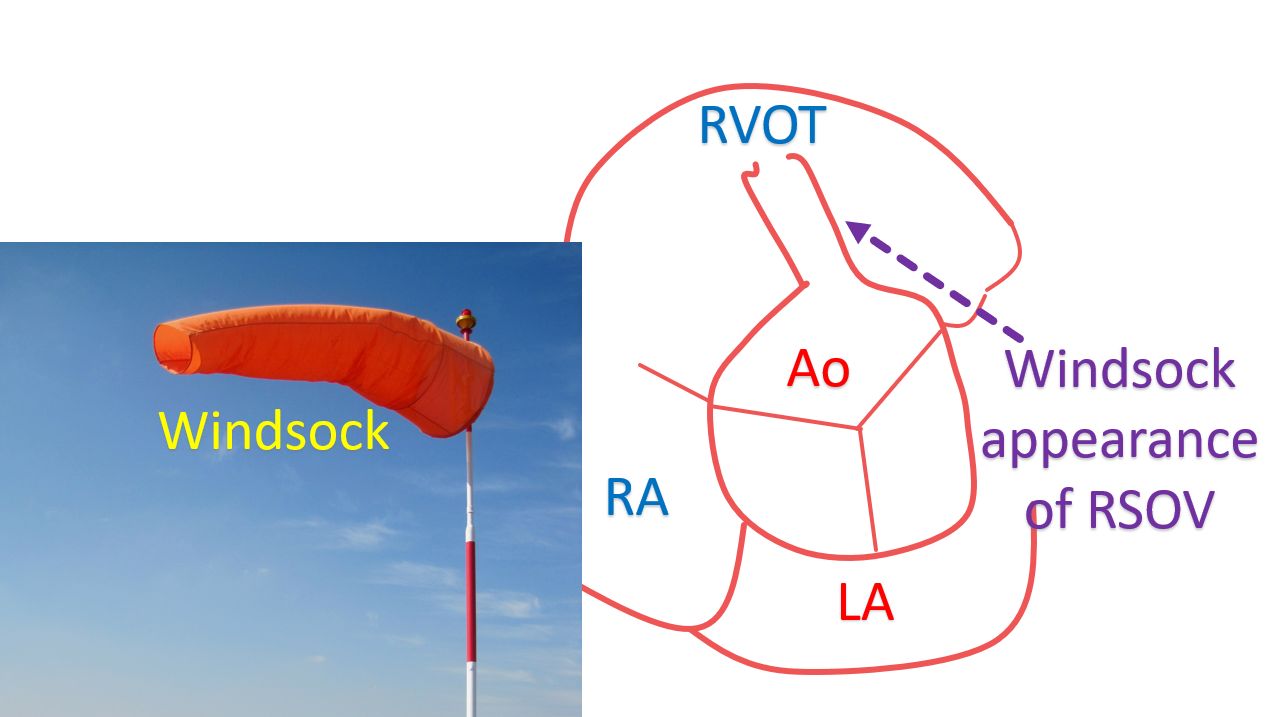
RVOT: right ventricular outflow tract; RA: right atrium; LA: left atrium; Inset shows an actual windsock in an airport.
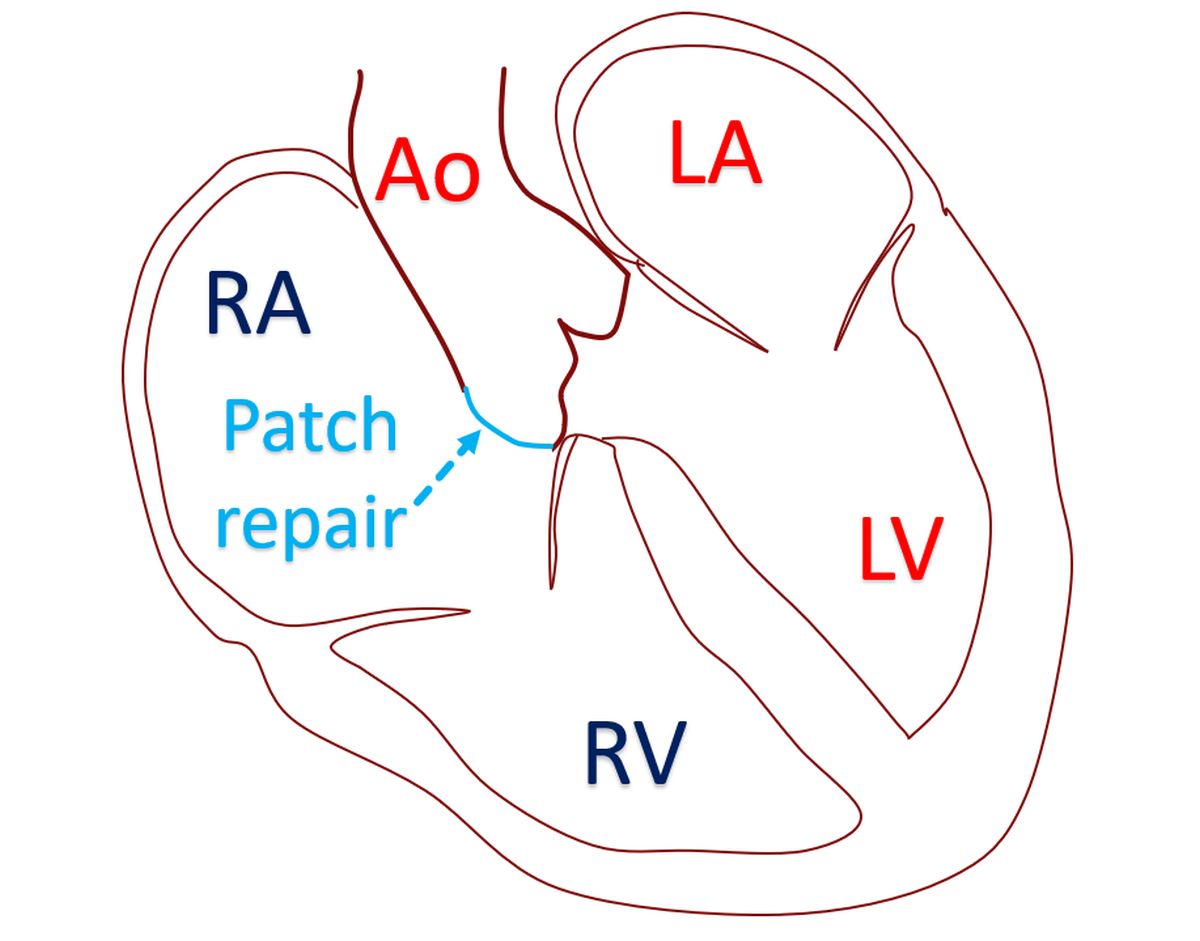
Conventionally, RSOV has been repaired surgically, with the first repair being done by Lillehei and colleagues in 1957. The aneurysmal sac is removed and the defect repaired either by direct stitches or patch closure. Associated defects like ventricular septal defect and aortic regurgitation will be tackled in the same surgical sitting. Aortic valve replacement may be needed in some cases. Ventricular septal defect is a hole in the wall between the two lower chambers of the heart. Aortic regurgitation is leak in the aortic valve, which is situated near the RSOV.
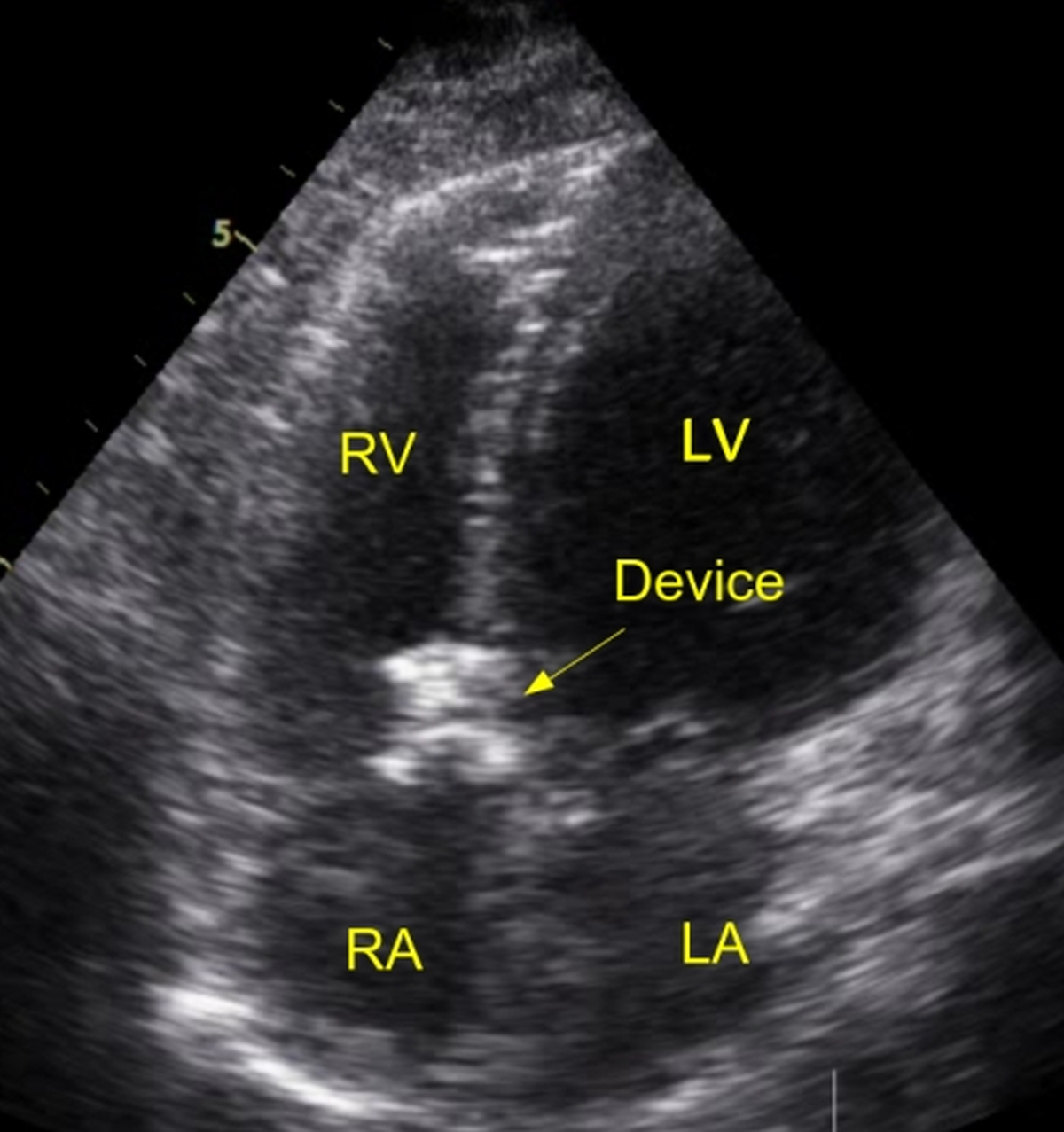
Device closure of RSOV is another option being increasingly used in suitable cases. The distance from the aortic end of the RSOV to the opening of the coronary artery is specifically measured to check whether the device will impede coronary flow to the heart muscle. In a report of 25 cases, a procedural success rate of 84% was achieved, including two patients who had come with very low blood pressure. The devices were implanted using small tubes introduced through the blood vessels of the groin, to which the device is attached. Two patients had residual leak and there was one case of device embolization. Embolization is dislodgement of the device and movement of the device along with the blood circulation into another region. In one case, there was device induced severe aortic regurgitation. Associated ventricular septal defect was closed simultaneously in one patient. Three patients were referred for surgery.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal