Tricuspid Regurgitation
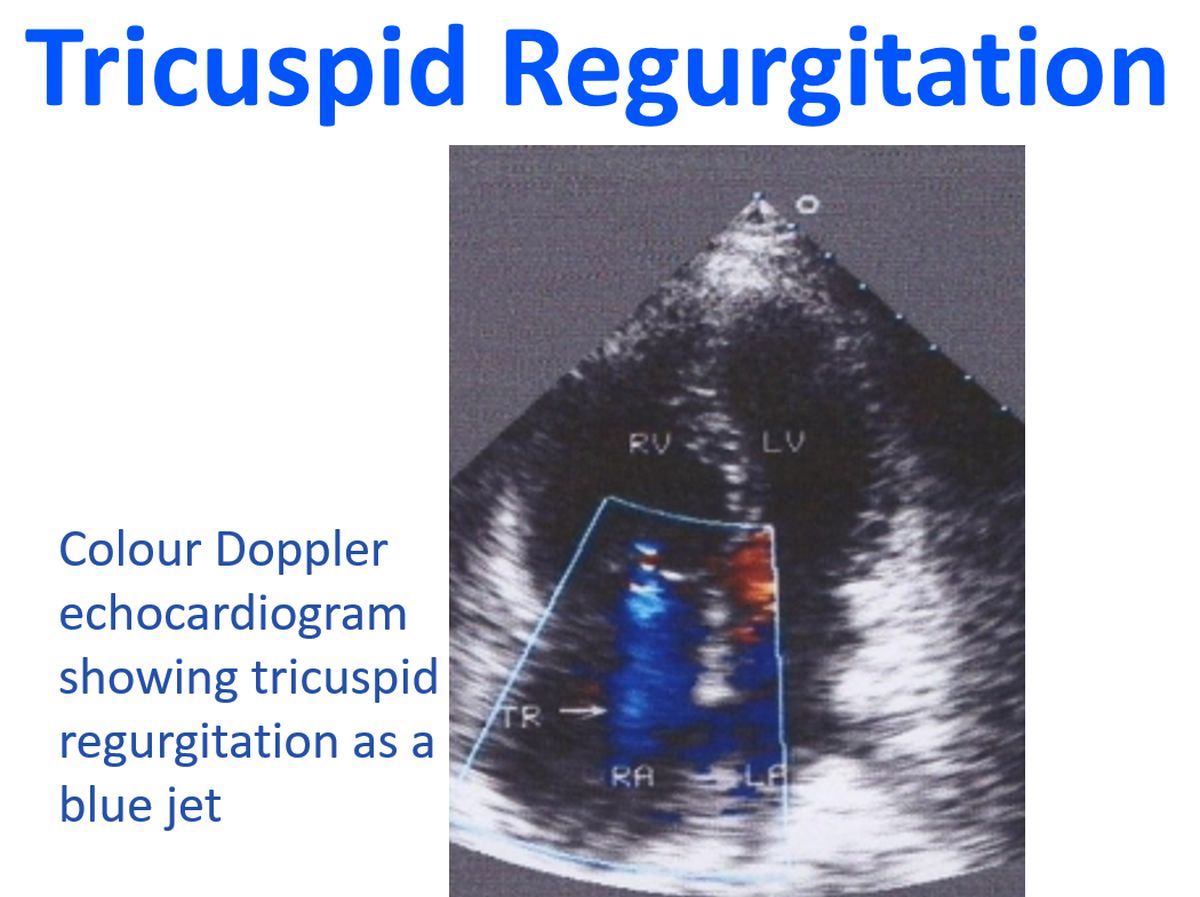
Tricuspid Regurgitation
Tricuspid valve is the largest of the four heart valves. Tricuspid regurgitation is most often secondary to elevated right ventricular pressure as a consequence of pulmonary hypertension. Hence it is often associated with other valvular disorders like mitral stenosis. In rheumatic heart disease, isolated TR will be very unlikely as the mitral valve will be invariably affected in such cases.
TR can be divided into hypertensive and non-hypertensive. Non-hypertensive TR occurs due to structural abnormalities of the tricuspid valve like Ebstein’s anomaly. Tricuspid valve endocarditis is also an important cause of tricuspid regurgitation, especially in intravenous drug abusers. TR is also a feature of carcinoid heart disease. Severe TR produces right atrial dilatation and a prominent V wave in the jugular venous pulse.
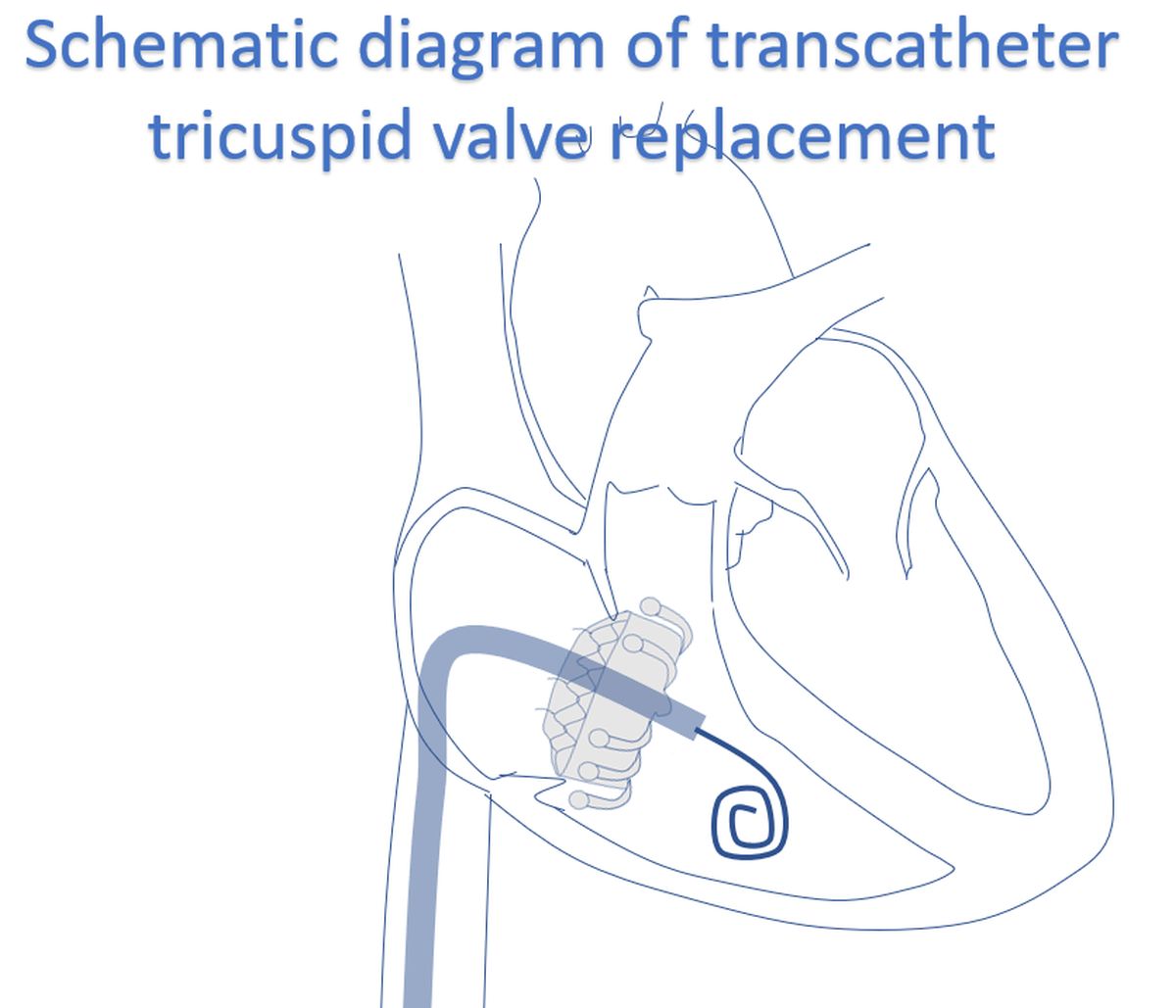
Severe TR may require surgical repair. de Vega’s annuloplasty is useful in controlling tricuspid regurgitation. Rare cases may require prosthetic valve replacement. Bioprosthesis is preferred in tricuspid location because of the tendency for thrombosis due to the low velocity of blood flow across the tricuspid valve. Unlike in the mitral and aortic position, degeneration of bioprosthesis is lesser in the tricuspid position due to lower hemodynamic load. Transcatheter tricuspid valve replacement is an evolving option in the treatment of tricuspid regurgitation.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal