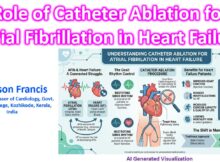
The management of atrial fibrillation (AF) in the setting of heart failure (HF) has undergone a major paradigm shift. The historical approach of rate control as a purely
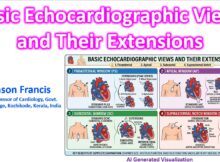
Assessing right ventricular (RV) function via echocardiography is uniquely challenging due to the chamber’s complex, crescentic geometry and its position immediately behind the sternum. Because no single two-dimensional
A complete Transthoracic Echocardiogram (TTE) relies on four primary acoustic windows to visualize the heart’s anatomy and hemodynamics. 1. Parasternal Long-Axis View (PLAX) The PLAX view is typically
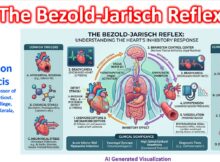
The Bezold-Jarisch reflex (BJR) is an inhibitory cardiovascular reflex originating from receptors within the heart itself. When triggered, it causes a classic triad of bradycardia (slow heart rate),
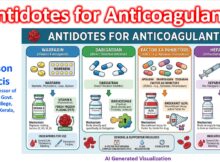
The management of life-threatening bleeding or the need for emergent surgical intervention in anticoagulated patients requires specific reversal strategies based on the drug class. Here is the quick-reference
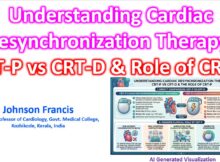
Both Cardiac Resynchronization Therapy (CRT) devices provide biventricular pacing to coordinate the contraction of the right and left ventricles. This corrects mechanical dyssynchrony, improves cardiac output, and reduces
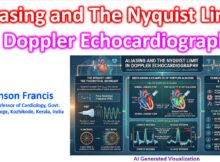
In Doppler echocardiography, aliasing is an artifact that occurs when the Doppler shift frequency exceeds the system’s ability to sample it accurately. The threshold at which this signal
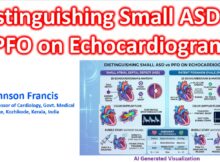
Distinguishing a small Atrial Septal Defect (ASD) from a Patent Foramen Ovale (PFO) on an echocardiogram hinges on identifying whether there is a true anatomical deficiency of septal
Question 1: Fundamental Principles Which of the following physical characteristics primarily distinguishes OCT from IVUS imaging?A) OCT uses high-frequency sound waves, whereas IVUS utilizes near-infrared light.B) OCT relies
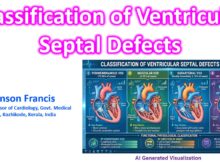
Ventricular septal defects (VSDs) are primarily classified based on their anatomical location within the ventricular septum—the wall separating the heart’s right and left lower chambers. Because the septum