2:1 AV Block and Right Ventricular Hypertrophy
2:1 AV block and right ventricular hypertrophy
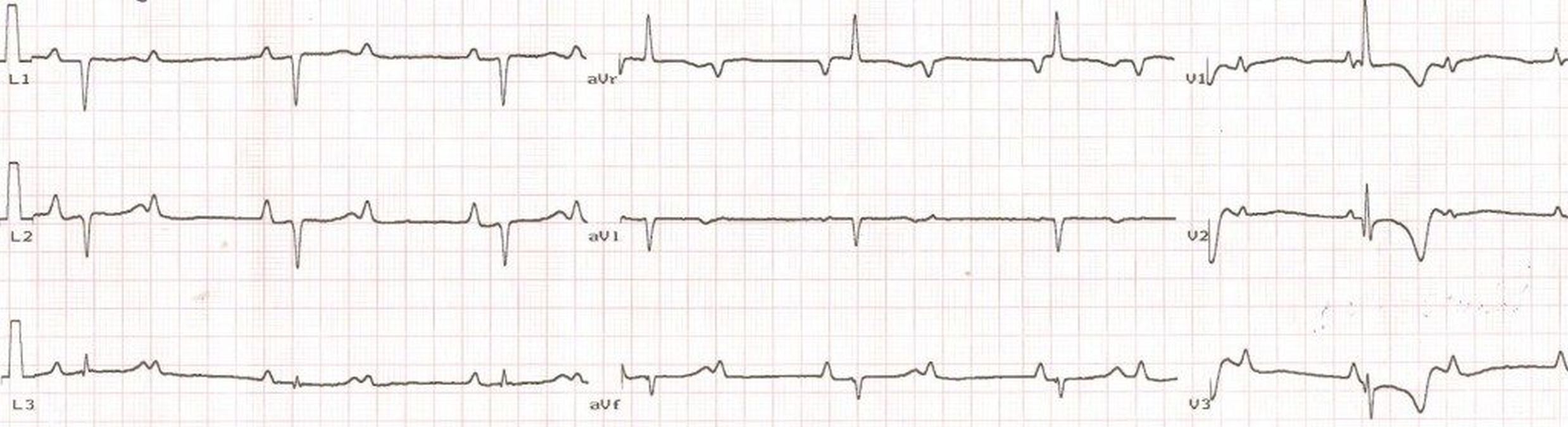
There are regular P waves at a rate twice that of QRS complexes, indicating 2:1 AV block (or 2:1 AV conduction). P waves are sharp in lead II, suggesting right atrial overload, which is also manifest as prominent positive deflection of P wave in V1. There is extreme right axis deviation with negative QRS complexes in lead I and aVF as well as positive QRS complexes in aVr. Prominent R waves in V1 and the right axis deviation are due to right ventricular hypertrophy. T wave inversion in V1 to V3 are possibly due to right ventricular strain. Another possibility which has to be considered is postanoxic T wave inversions which can occur after a Stokes – Adam attack which can occur due to intermittent complete heart block.
A combination of right bundle branch block and right posterior hemiblock can also produce a similar QRS pattern, but the QRS width will be more in that case. Endocardial cushion defects can be considered in the etiology as such a situation can occur if there is AV block and pulmonary hypertension due to a ventricular septal defect. L-transposition may also be thought of as there is a small q wave in V1 while there were none in V6, though not captured in this image. But the q in V1 can very well be explained by right ventricular hypertrophy.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal