Aortic Stenosis – narrowing of the valve between left ventricle and aorta
Aortic Stenosis – narrowing of the valve between left ventricle and aorta
Aortic valve is the valve between the aorta and left ventricle, preventing backflow of blood into the left ventricle from the aorta. Aortic stenosis, narrowing of the aortic valve can be congenital i.e., present at birth or acquired.
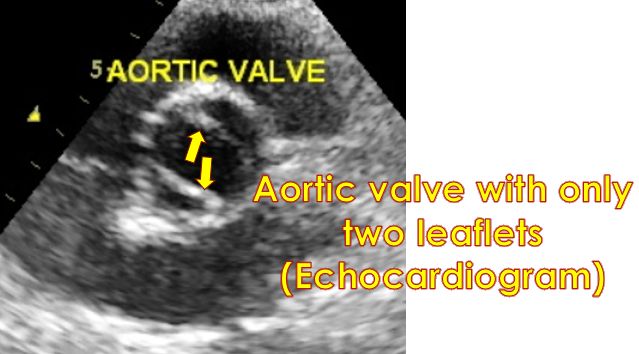
Congenital aortic stenosis is often secondary to degenerative changes in a bicuspid aortic valve. Normal aortic valve has three cusps.
Calcific aortic stenosis of the elderly is related to dyslipidemia or increased levels of fat like cholesterol in blood and atherosclerosis or damage to blood vessels due to aging and fat deposition.
Rheumatic fever is an important cause for aortic stenosis in the developing countries. Rheumatic aortic valve disease is often a combination of stenosis and regurgitation or leak.
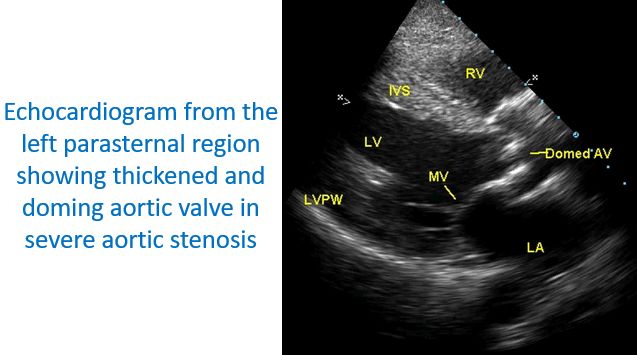
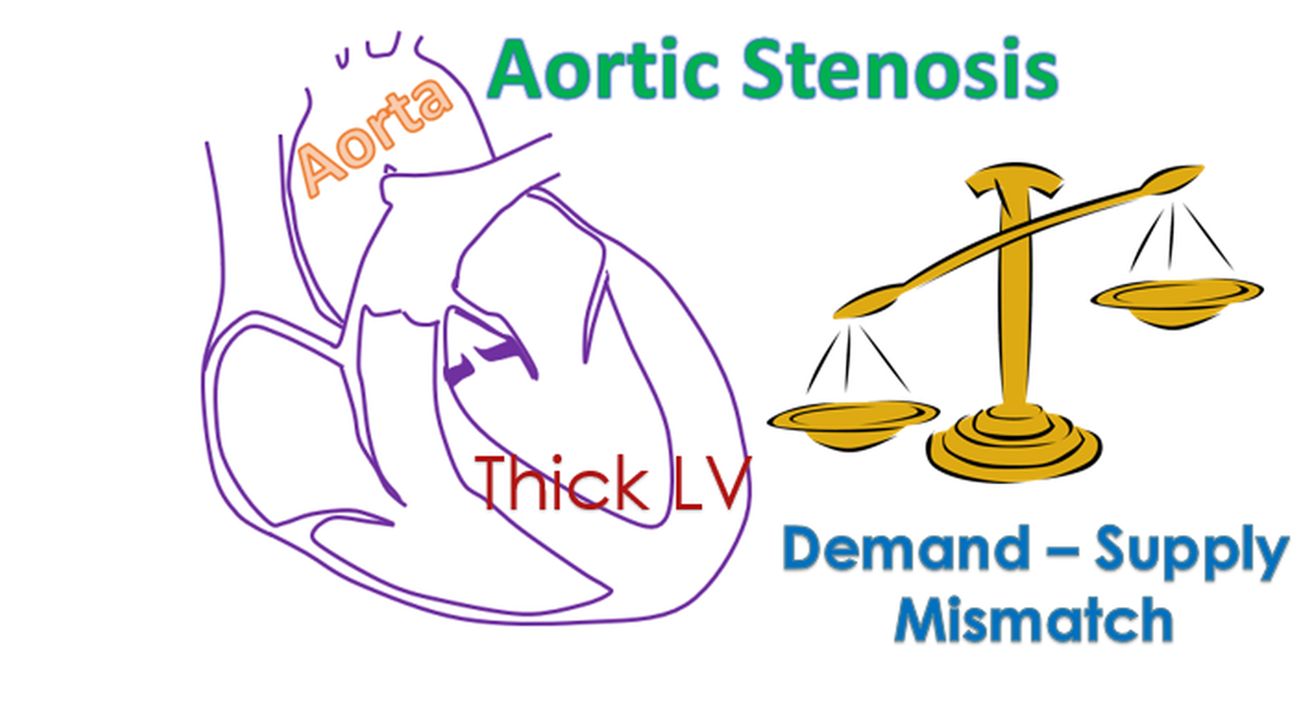
Severe aortic stenosis causes left ventricular hypertrophy, thickening of the walls of the left ventricle, lower muscular chamber of the heart and angina pectoris. Angina pectoris is chest pain due to decrease supply of oxygenated blood to the heart as a result of coronary demand – supply mismatch.
When a person with severe aortic stenosis exercises, syncope can occur due to the fixity of cardiac output. Peripheral vasodilatation or dilatation of the peripheral blood vessels with exercise leads to shunting of blood away from the brain and syncope.
ECG shows left ventricular hypertrophy with strain pattern, an ECG pattern seen when the left ventricle faces a pressure overload, in severe aortic stenosis. Severity of aortic stenosis can be assessed by Doppler echocardiography or ultrasound imaging of the heart.
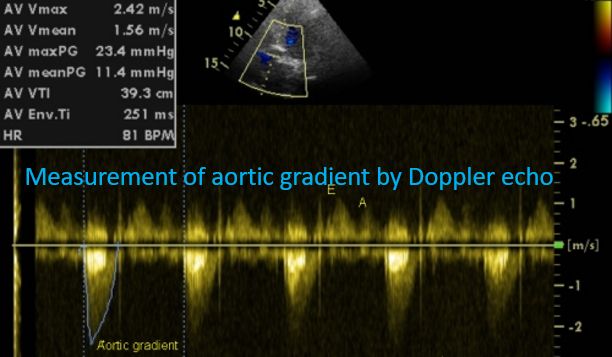
Transvalvular gradient across the valve above 75 mm Hg is considered as severe aortic stenosis. Gradient can be falsely low with the onset of left ventricular dysfunction, reduced pumping function of the heart due to disease.
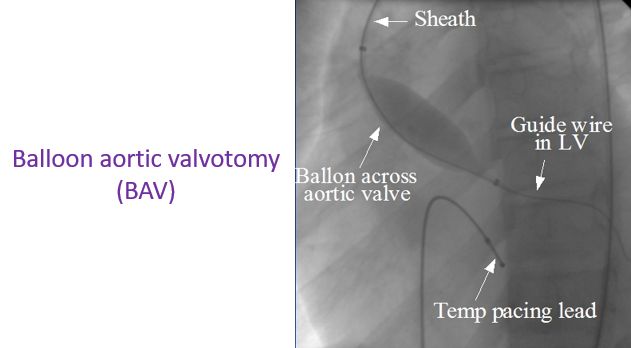
Severe aortic stenosis can sometimes be treated by balloon valvotomy, opening of the narrowed valve by inflation of a balloon kept within it. It is often as a palliative treatment.
The definitive treatment required is aortic valve replacement. Replacement can be done with mechanical valve or bioprosthetic valve.
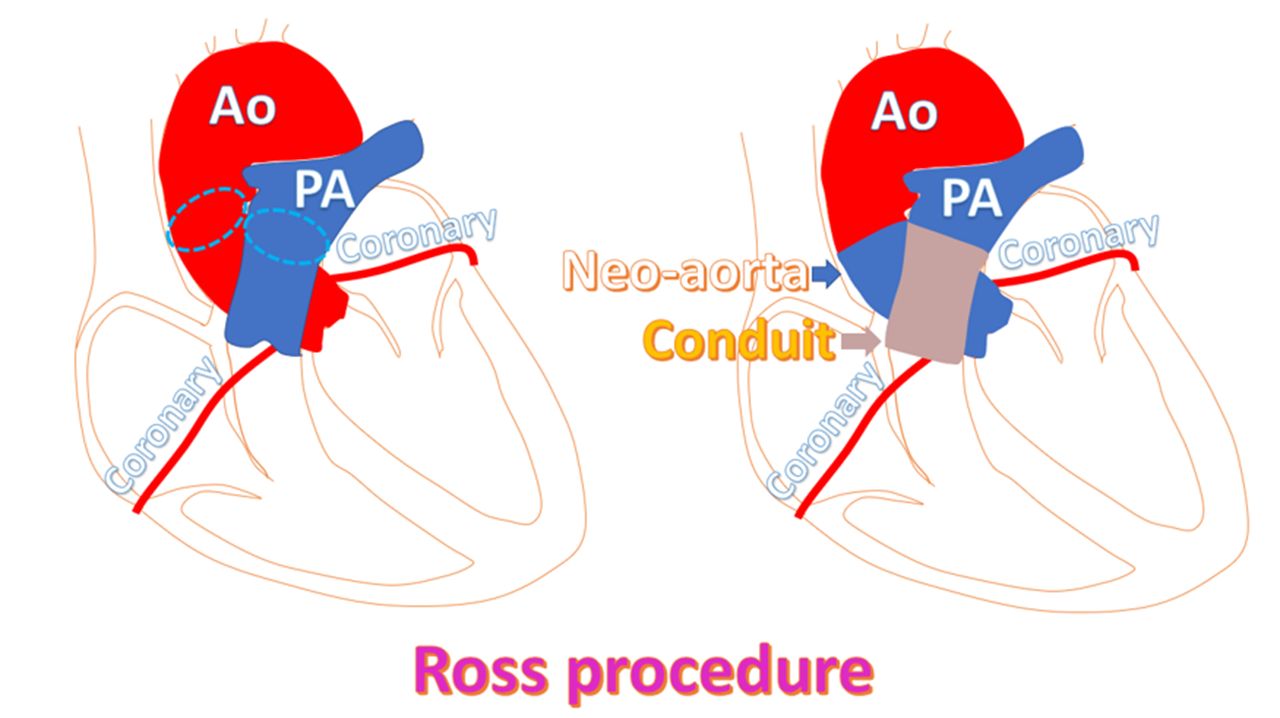
In young children and adults, pulmonary autograft known as Ross procedure is preferred.
Mechanical prosthesis requires life-long anticoagulation, medicines to prevent clotting of blood.
Those on anticoagulant medications need to monitor the clotting function of the blood on a regular basis to achieve optimal dosage to prevent complications.
Trans catheter aortic valve implantation known in short as TAVI is a novel method for the treatment of aortic stenosis. A prosthetic valve is mounted on a small tube and delivered in the location of the valve through small openings made in the skin.
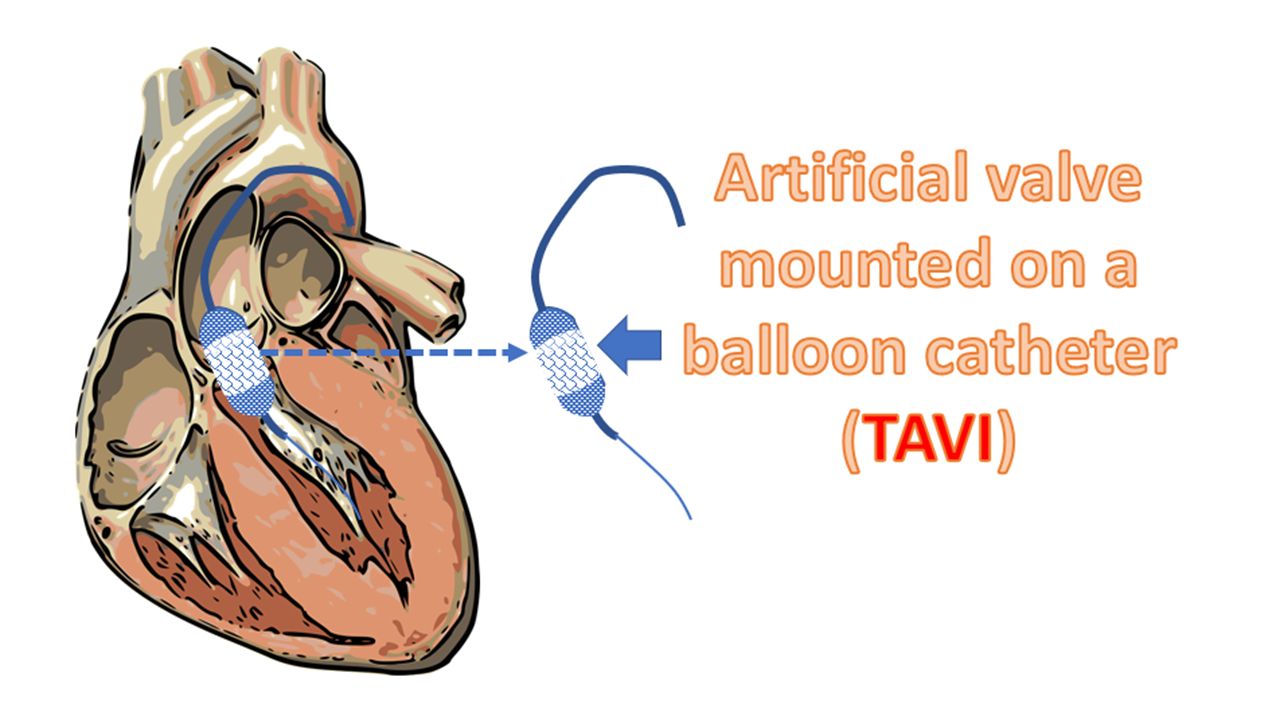
It can be delivered directly to the heart using a tiny opening over the left side of the chest or indirectly through an opening in the groin. In the latter case, it is passed along the femoral artery, blood vessel in the thigh, upwards into the aorta.
The device is advanced under X-ray fluoroscopic visualization and positioned across the narrowed valve before it is inflated to achieve actual desired size. Though initially considered only for high surgical risk patients, TAVI is now being considered for younger and lower surgical risk patients as well.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal