Atrial septal defect (ASD) – hole in the wall between two upper chambers of the heart
Atrial septal defect (ASD) – defect in the interatrial septum
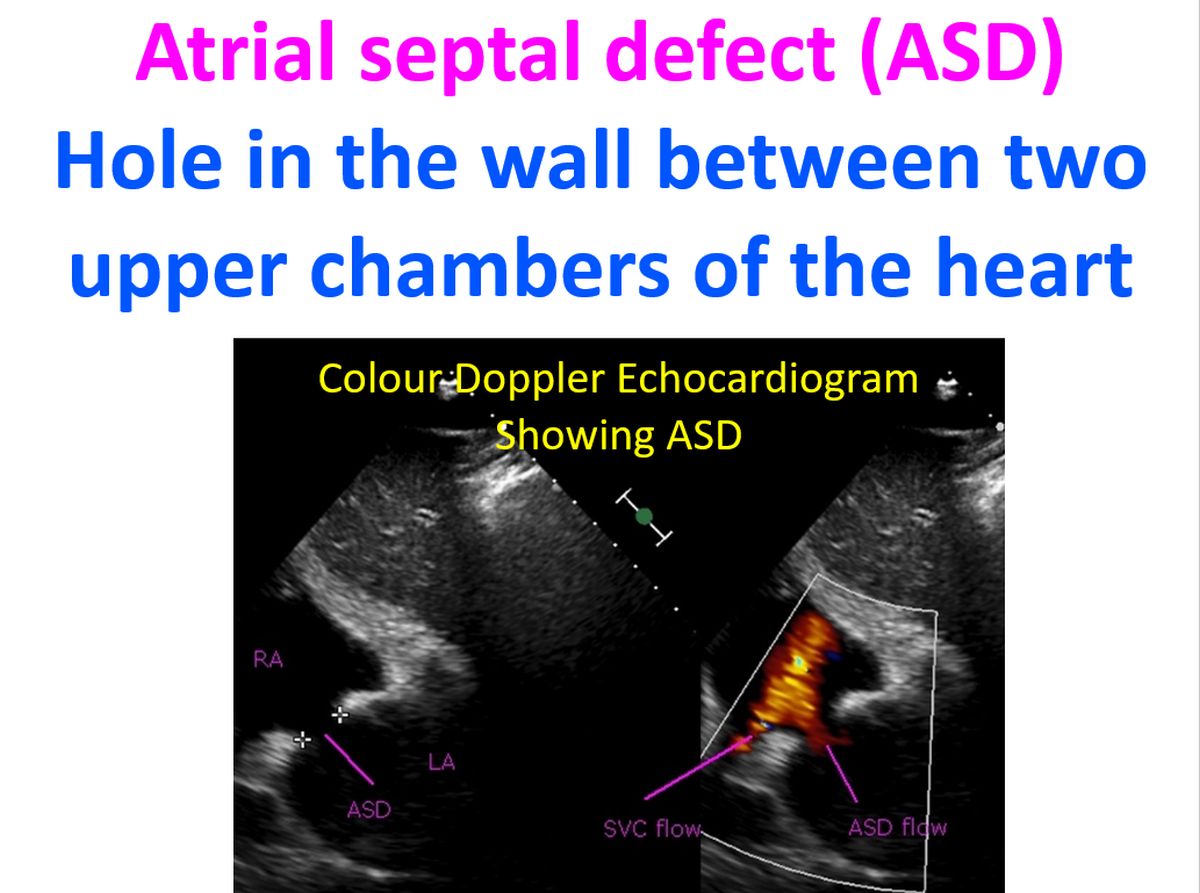
Atrial septal defect is one of the commonest congenital heart diseases in the adult. It is a defect in the septum separating the two upper chambers of the heart. The defect in the septum between right and left atrium can be in various locations. The commonest variety which occurs almost in the centre is known as ostium secundum type. If it occurs at the lower end, it is called ostium primum ASD.
Ostium primum ASD is often associated with a cleft of the mitral valve and leakage of the mitral valve (mitral regurgitation). Sometimes there can be tricuspid regurgitation as well. There is another type of defect known as sinus venosus ASD. Sinus venosus ASD can occur near the superior vena cava or inferior vena cava. The former is more common than the latter and can be associated with defects in the sinus node, the pacemaker of the heart situated nearby.
ASD leads to shunting of blood from left atrium to right atrium as the latter is at a lower pressure. This increases the blood flow to the lungs. Increased flow leads to dilatation of pulmonary vessels and in the long term reactive pulmonary hypertension. When the pressure in the blood vessels increase in the long run due to long standing increased flow, it increases the pressure in the right ventricle and thickening of the right ventricular muscles. This leads reduced compliance of the right ventricle and raises the diastolic pressure in the ventricle. This rising pressure is transmitted to the right atrium so that right atrial pressure rises above the left atrial pressure.
The higher pressure causes a reversal of the shunt and right to left shunt occurs. This means that deoxygenated blood from the right atrium reaches the left atrium and mixes with oxygenated blood in the left atrium. Blood from left atrium moves to left ventricle and aorta. So the blood reaching all organs become less saturated with oxygen. This manifests as cyanosis (bluish discolouration of skin and lips). This situation of reversed shunt in an ASD with cyanosis due to desaturated blood reaching the organs is known as Eisenmenger Syndrome.
Atrial septal defect can be closed by procedures if detected in childhood. Some of the ASDs detected in infancy may close spontaneously, especially the smaller ones. Those ASDs remaining after 3 – 5 years can be closed either by device closure or surgery. Surgery is an open heart surgery with support from heart lung machine. ASD device closure is done through the veins which drain blood to the heart. Usually the femoral vein in the thigh is entered under local anaesthesia (general anaesthesia in a small child). The guide wire is taken to the heart under X-ray fluoroscopic guidance.
A sheath is introduced over the wires across the defect into the left atrium and the pulmonary vein. The device occluder is introduced through the sheath and delivered across the defect using fluoroscopic guidance and confirmation by simultaneous transesophageal echocardiography (ultrasound imaging done with a device introduced into the esophagus, the food pipe). When the device occluder is used, the person can walk about the next day and return home. There is no wound in the chest, only a tiny puncture in the groin where the sheath was introduced.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal