Bundle Branch Blocks and Hemiblocks
Bundle Branch Blocks and Hemiblocks
Left bundle branch block (LBBB) is characterized by a wide QRS complex with a slurred R wave in V6 and slurred negative wave in V1 (QS complex). The initial r wave in V1 and the initial q wave in V6 which represents the initial left to right activation of the septum are absent in LBBB.
Right bundle branch block (RBBB) is characterized by rSR’ pattern in V1 and Rs pattern with slurred s in V6. The initial r in the rSR’ pattern will be lost if there is coexistent anterior wall myocardial infarction, resulting in a QR pattern. This pattern is also called QRBBB. Presence of RBBB in a patient with anterior wall myocardial infarction indicates that the extent of myocardial infarction is more. These patients are prone for left ventricular dysfunction.
Left anterior hemiblock (LAHB) is characterized by rS pattern in II, III, aVF and qR pattern in I and aVL. This results in left axis deviation. LAHB is a common accompaniment of anterior wall myocardial infarction. The presence of LAHB does not significantly worsen the prognosis in patients with anterior wall infarction. LAHB is also associated with several congenital heart diseases like ostium primum ASD and tricuspid atresia.
Left posterior hemiblock (LPHB) is characterized by rS pattern in I, aVL and qR pattern in II, III, aVF. This results in right axis deviation. If LPHB is associated with anterior wall myocardial infarction it carries a poor prognosis. This is because left posterior fascicle is spread over a larger area and is affected only in more extensive infarction. Moreover, left posterior fascicle has dual blood supply and its involvement may suggest multi-vessel coronary artery disease.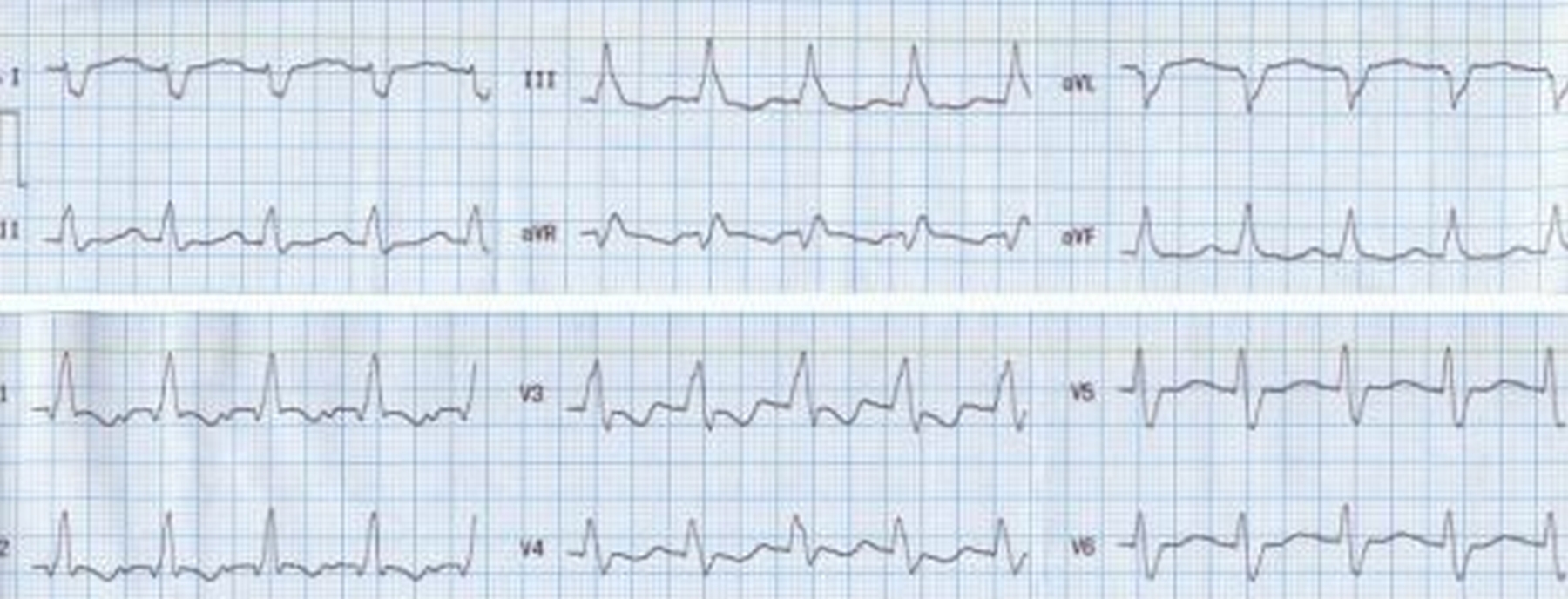
ECG showing RBBB, LPHB
Some authors have also described a left septal fascicular block [1].
Reference
- MacAlpin RN. Left septal fascicular block: myth or reality? Indian Pacing Electrophysiol J. 2003 Jul 1;3(3):157-77.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal