Chest X-ray – overview
Chest X-ray – overview
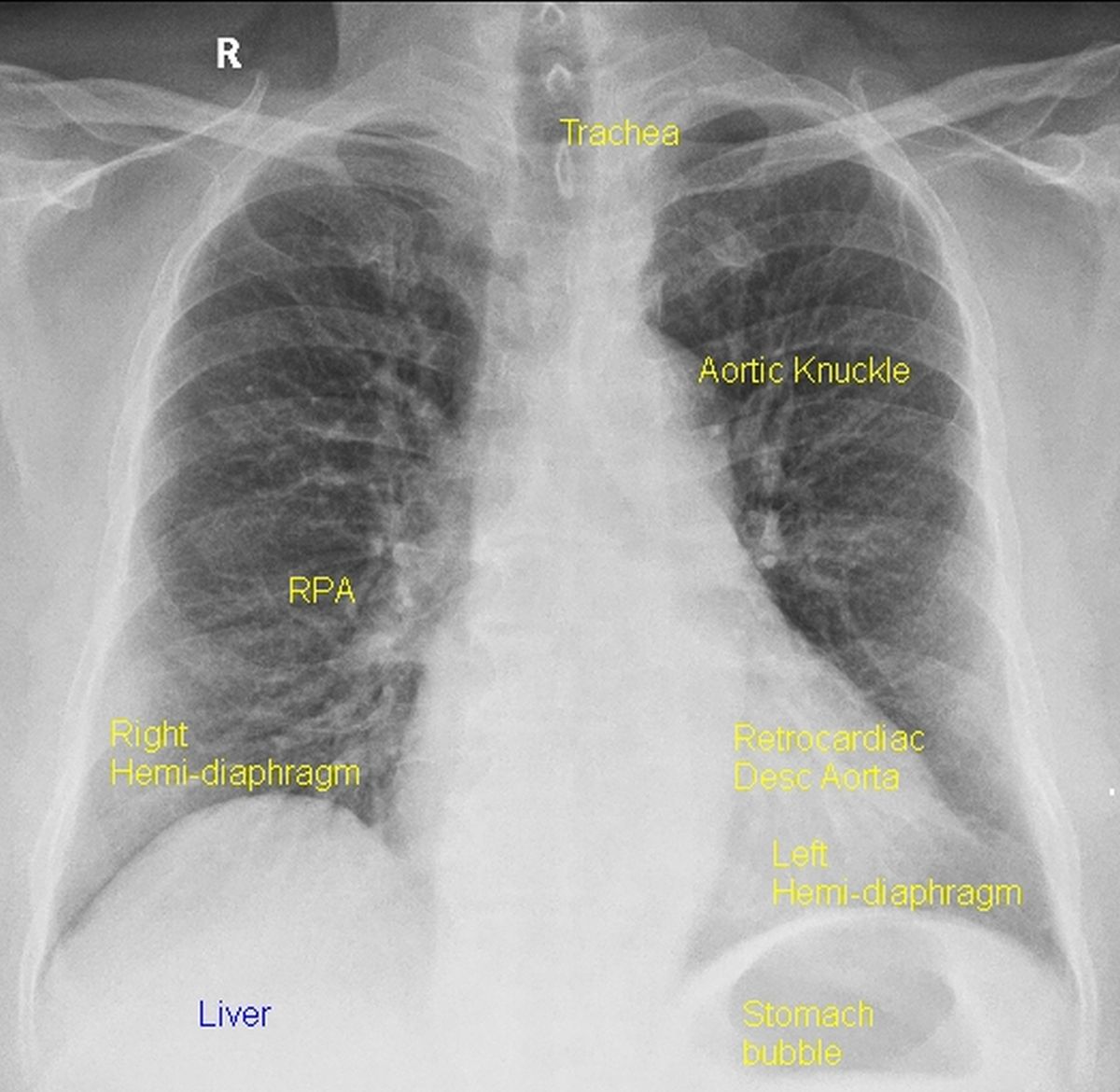
Chest X-ray (CXR) PA view (Figure 7.1) is the one routinely taken for cardiac evaluation. Lateral view and oblique views are rarely taken in specific situations. But interpretation of these views is more challenging than the PA view, mainly because of lack of familiarity due to lower usage.
CXR PA view is taken with the tube-film/sensor distance of 6 feet in the erect posture. Care is taken to keep the scapulae away from the lung fields by appropriate positioning. Standard imaging is done in held inspiration. These details are important to avoid artifactual enlargement of the cardiac silhouette. With a proper penetration level spines of upper three thoracic vertebrae are visible while the lower ones are blurred. More vertebral spines are visible in an over penetrated view.
It is conventional to start reading by checking the side label so as not to miss a dextrocardia with inverted film. Next comes soft tissue and bony cage. In a well-positioned CXR without rotation, the medial ends of the clavicles are equidistant from the midline.
Lower border of ribs may show notching (Dock’s sign) in coarctation of aorta due to erosion by collaterals. Rib notching is usually bilateral and seen on ribs 3-8. It can also be unilateral in certain other conditions. Thin translucent layer of air surrounding the mediastinum (pneumomediastinum) is a rare finding which can be easily missed. A hydropneumopericardium is a still rarer finding which manifests as an air fluid level within the cardiac silhouette.
Horizontal extent of the cardiac shadow divided by the internal transverse extent of the thorax above the diaphragm gives the cardiothoracic ratio, which is less than 50% normally. Tracheal shadow and its division are important to check the visceral situs. The right bronchus is more vertical than the left bronchus. The left bronchus gets elevated with left atrial enlargement, widening the subcarinal angle.
Aortic knuckle is seen at upper end of the left cardiac border. Major part of the left border is the left ventricle. Right border is formed by the right atrium. Right hemidiaphragm is the upper limit of the liver shadow. Left hemidiaphragm is above the stomach bubble. The location of these are important in identifying the visceral situs. Major part of the heart shadow is in the left hemithorax with apex in the left lower part. This is reversed in dextrocardia.
Normally main pulmonary artery segment is in the concavity below the aortic knuckle (Pulmonary bay). Left descending pulmonary artery is behind the cardiac shadow, parallel to the descending thoracic aorta. Right descending pulmonary artery is seen lateral to the right bronchus air shadow. Pulmonary vessels are prominent in the lower zones due to the effect of gravity.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal