Determination of QRS axis
Determination of QRS axis
Mean QRS axis is also often called the mean electrical axis of the heart. A simple way to assess whether the mean QRS axis is normal or not is to look at leads I and aVf. If the average QRS deflection (difference between the amplitude of positive deflections and the negative deflections) is positive in both leads, the QRS axis is normal, i.e., between 0 degrees and +90 degrees. The electrical axis of lead I is 0 and that of aVf is +90 degrees. To get a better approximation of the QRS axis, the average amplitude of QRS in lead I is plotted along X – axis and that in aVf is plotted along the Y – axis. The resultant of these two vectors will give the QRS axis. If the vector is in the left lower quadrant, the QRS axis is considered normal. QRS vector in left upper quadrant is considered left axis deviation if it is beyond -30 degrees from the horizontal. QRS axis in the right lower quadrant indicates right axis deviation. QRS vector in the right upper quadrant is either extreme right axis or extreme left axis deviation. It is also sometimes called north west axis or indeterminate axis.
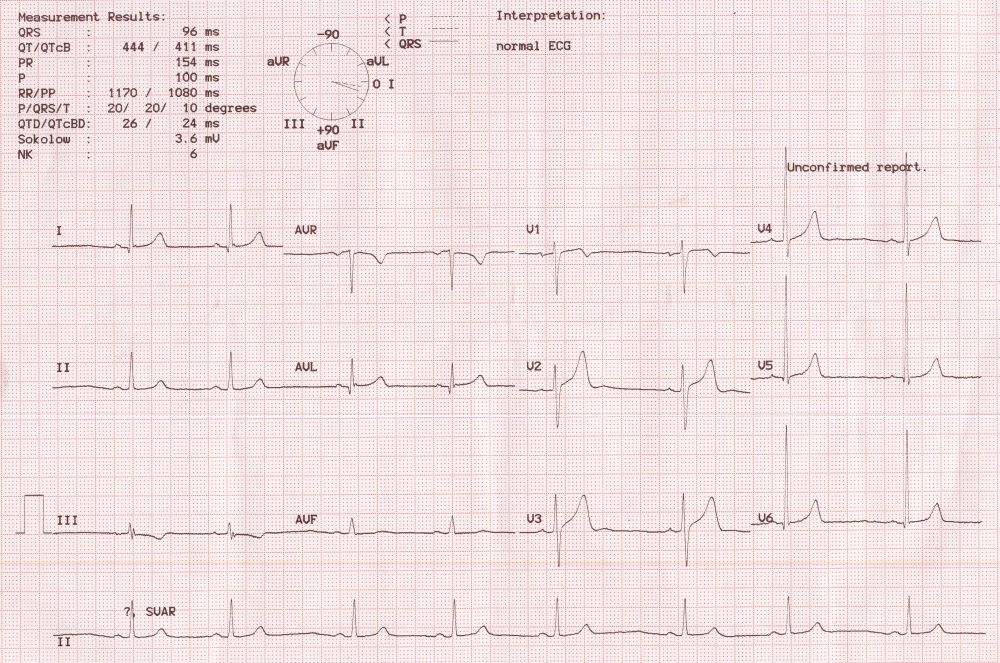
It is not practical to determine the QRS axis by plotting the vector in a bedside setting in which ECGs are often evaluated. Usual method of bedside determination of QRS axis is by looking at the lead in which QRS complex is biphasic or having smallest amplitude. The mean QRS axis will be perpendicular to the axis of that lead. For this a knowledge of the axis of each of the lead is essential. The positive pole of lead I (left arm) is taken as the zero reference (0 degrees). The negative of lead I (right arm) will become + / -180 degrees. The positive pole of aVf is taken as +90 degrees and negative pole of aVf is -90 degrees. Positive of aVl is -30 degrees and negative +150 degrees. Since the QRS complex in aVr is negative normally, if the maximum negative deflection is in aVr it will indicate a QRS axis of +30 degrees. If the maximum positive deflection is in aVr, it will indicate a QRS axis of -150 degrees. Similarly, the positive pole of lead II is 60 degrees and the negative pole -120 degrees. Positive pole of lead III is +120 degrees and the negative pole -60 degrees. This system of checking the QRS axis with respect to the six limb leads is known as the hexaxial reference system. If two leads show almost same QRS amplitude, which is also the maximum QRS amplitude in the limb leads, then the axis is considered to be between those two leads. For example, if leads II and aVf show the tallest QRS complexes, then the QRS axis will be approximately +75 degrees. This will also mean that the shortest QRS complex will be seen in the leads with a perpendicular axis i.e., leads I and aVl. Sometimes it may not be the shortest QRS complexes, but a transition from positive to negative complexes between these leads.
The same technique can be used for determination of P wave and T wave axis, though it is seldom done in clinical practice. Normally these vectors are in the same direction with only a small angle between them. A widening of the QRS – T angle indicates a change in the depolarisation – repolarisation sequence.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
I have a rather basic question, Dr. Francis, but one that I’ve been unable to find an answer for. As I understand it, a vector that is perfectly perpendicular to a lead can inscribe a QRS that is either perfectly biphasic (or equiphasic) or one that is isoelectric (zero amplitude, flat baseline). I was told by one electrophysiologist that a perfectly perpendicular vector must always show a deflection, either positive or negative, as long as there is an electrical charge involved. Yet I find other references in the literature to perpendicular vectors resulting in isoelectric lines. Can a perpendicular vector cause both, and if so, why at times one rather than the other?
Just in reply to the question above (albeit 4 years late!), my understanding is that the definition of isoelectric is to have no net charge. So although isoelectric can refer to a flat baseline, it can also refer to a true biphasic wave as there is also no net charge of a bisphasic wave.
Thanks for the post (albeit 4 years late!). I came to the same conclusion that it was all an issue of NET charge which would make an isoelectric deflection the equivalent of an equiphasic deflection.
Still reading this blog. Best wishes,
Jerry W. Jones MD FACEP
A big thanks to both of you!