Diagnosis of hypertrophic cardiomyopathy
Diagnosis of hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is a genetic disorder with a guarded prognosis which occurs in about 1:500 individuals. Echocardiography is the sheet anchor of diagnosis of HCM and other modalities are complementary. It is an autosomal dominant disorder with variable penetrance with either a defect in sarcomeric protein genes which encode for myosin heavy chain, actin or tropomyosin or due to abnormal myocardial Ca++ kinetics which increase intracellular Ca++, causing hypertrophy and cellular disarray.
MYH7 mutation in the gene which encodes for beta myosin heavy chain, located on chromosome 14 is found in about 15-25% of cases of HCM. MYBPC3 which encodes for cardiac myosin binding protein C is abnormal in another 15-25% cases. Besides these several other mutations have been described, some of which are available commercially for testing.
There are several phenocopies of HCM, caused by other disorders like Barth syndrome, Danon’s syndrome, Pompe’s disease, Fabry’s disease, Friedreich’s ataxia and Noonan’s syndrome. Genetic markers for some of these disorders are also available commercially.
Sigmoidal HCM which is about 40-50% has about 10% positivity for myofilament gene. Reverse curve HCM occurs in 30-40% cases, and has a myofilament gene in 80% of them. Apical HCM and neutral HCM (with symmetric hypertrophy) contributes 10% each, and has 30-40% positivity of myofilament gene.
Symptoms of HCM include syncope / near syncope, which could be precipitated by exertion, hypovolemia, rapid standing, Valsalva manoeuvre, diuretics, vasodilators or arrhythmia. The most common symptom is dyspnoea which occurs in 90% of cases and is due to elevated left ventricular diastolic pressures as a consequence of the diastolic dysfunction. Palpitations can be felt if there are arrhythmias. Angina is another common symptom due the hypertrophy which causes a coronary supply demand mismatch.
Physical signs in HCM
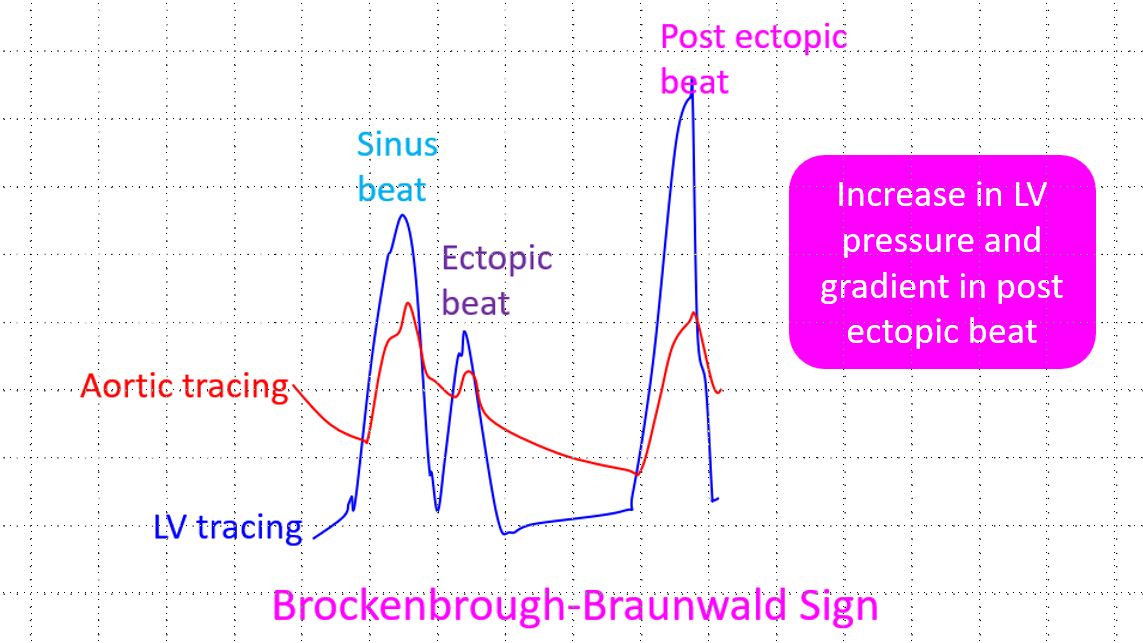
The carotid pulse is jerky and may have dual peaks. But the second peak is often appreciated only in a pulse tracing rather than on palpation, because it is somewhat rounded. Jugular venous pulse may show a prominent a wave. Double or triple apical impulses can be felt in HCM. In case of triple impulse, it is one diastolic (due to forceful atrial contraction) and two systolic impulses (due to mid systolic obstruction). Paradoxical splitting of second heart sound can occur due to the left ventricular outflow tract obstruction (LVOTO). A third heart sound occurs when the left ventricle decompensates in late stages of HCM. A prominent fourth heart sound is usual in HCM due to the diastolic dysfunction which causes forceful atrial contraction. Dynamic auscultatory features are important in the diagnosis of HCM. The systolic ejection murmur increases with a decreased preload as in volume depletion, nitrate therapy or standing or a decreased afterload with vasodilators. The murmur decreases with an increase in preload or afterload (isometric hand grip). The post ectopic increase in the murmur is a hallmark of hypertrophic obstructive cardiomyopathy, which differentiates it clinically from mitral valve prolapse.
ECG changes in HCM
ST-T wave abnormalities are common, with ST segment depression and T wave inversion predominating. Left ventricular hypertrophy, left atrial enlargement, QRS axis deviation (left > right), conduction abnormalities like increased P-R interval and bundle branch block may be noted. Atrial fibrillation if present indicates poor prognosis as hemodynamic decompensation occurs due to loss of atrial booster action which is vital for the filling of a hypertrophied left ventricle with severe diastolic dysfunction.
Echocardiography in HCM
Important echocardiographic features include mitral regurgitation and LVOTO. The ejection fraction (EF) is high to normal, except in late decompensated stage. Small left ventricular (LV) cavity and left atrial enlargement are other features.
Septal thickness is often 4-6 mm more than normal. Asymmetric septal hypertrophy with absolute thickness more than 15 mm, septal / posterior wall (PW) ratio > 1.3 in normotensives and > 1.5 in hypertensives are some of the features. Rarely normal septal thickness can occur in genotype +ve cases, especially in cardiac troponin T mutations. Normal echo earlier in life can occur in cardiac myosin binding protein C mutation, which mandates repeat echo evaluation after five years. Apical hypertrophy can produce an ace of spades configuration of the LV cavity.
While assessing the severity of HCM, maximal wall thickness in multiple segments, length of septal hypertrophy, extension to apical segments and involvement of papillary muscles – anterior displacement / direct insertion into mitral valve have all to be looked into.
SAM in HCM
SAM (systolic anterior movement) of mitral valve occurs in 30 – 60%, but it is not specific. SAM causes LVOTO, increased ejection time and a decreased stroke volume, as well as mitral regurgitation due to poor coaptation of the leaflets. Severity of SAM can be quantified by septal contact time. In mild cases it is <10% and in severe cases it is >30% of systole.
LVOTO in HCM
Peak gradient > 30 mm Hg predicts (SCD) in HCM, though the gradients may be much higher in some cases.
LVOTO is due to septal hypertrophy, SAM and anterior displacement of mitral valve apparatus.
Mid cavity obstruction in HCM is associated with apical aneurysm, systemic embolism and arrhythmias. Cases are on record, in which ablation of the fourth septal artery has been done to ameliorate the obstruction in mid cavity obstruction.
Dynamic gradient in HCM
Dynamic gradient occurs in 25-30% and depends on blood volume / contractile state. Dynamic gradient may be sought by glyceryl trinitrate (GTN), Valsalva manoeuvre, standing position or even symptom limited exercise. Obstruction may occur during recovery and post exercise monitoring of gradient is mandatory.
False negative echo in HCM
Distal or apical hypertrophy may be missed and is best estimated on sequential short axis views.
Wall thickness may be normal in children and adolescents, cardiac troponin T mutations as well as in end stage HCM with dilated LV.
False positive echo in HCM
Oblique cut / foreshortened views and sigmoid septum in elderly can cause false positive diagnosis of HCM.
Thin posterior wall in inferior wall myocardial infarction (IWMI) causing abnormal ratio septal to posterior wall ratio can also cause suspicion of ASH (asymmetric septal hypertrophy).
LVOT gradients in hyperdynamic states may also be mistook for LVOTO in HCM.
Differential diagnosis of HCM
Differential diagnosis is not just by echo, but there is vital role for history and clinical examination. Hypertensive heart disease is an important differential diagnosis, but SAM is rare in this situation and there is evidence of greater diastolic dysfunction in HCM. Athlete’s heart is another entity with hypertrophy which may be confused with HCM. Normal / supernormal TDI (tissue Doppler imaging) velocities in athletes heart contrast with impaired velocities in HCM. LV cavity dilatation is seen in athlete’s heart. Cardiac amyloid is manifested with thickened interatrial septum, increased myocardial echogenicity and thickening of valve leaflets.
Radionuclide study in HCM
Radionuclide study has a limited role in HCM, mainly for documenting the absence of coronary artery disease (CAD). Thallium-201 scan may show an increased apical uptake.
Cardiac cath
Cardiac cath also has a limited role in the diagnosis of HCM in this era of echocardiography. Degree of outflow obstruction can be documented along with the classical Brockenbrough-Braunwald-Morrow sign. Evaluation of diastolic characteristics of LV and LV / coronary anatomy evaluation are other diagnostic uses of cath in HCM. The role of cath now a days is mostly for septal ablation.
Holter monitoring
Holter monitoring is useful to document nonsustained atrial / ventricular arrhythmias which may not be obvious clinically.
Contrast enhanced MRI (magnetic resonance imaging):
Delayed enhancement on contrast enhanced MRI is useful in documenting fibrosis in HCM, which is a predictor of systolic dysfunction and has a relation to heart failure symptoms.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal