Different ways of measuring cardiac output
Measuring cardiac output (CO) is a cornerstone of hemodynamic monitoring, moving historically from highly invasive gold standards to modern, non-invasive digital approximations.
The primary clinical modalities are categorized by their level of invasiveness, mechanism, and mathematical principles.
1. Invasive Methods (The Traditional Standards)
A. The Direct Fick Principle
Based on the law of conservation of mass, it assumes that the rate of oxygen consumption (VO2) by the body is equal to the amount of oxygen taken up by the lungs.
- The Formula: CO = VO2/(CaO2 – CvO2)
- Where CaO2 is arterial oxygen content and CvO2 is mixed venous oxygen content (sampled from a pulmonary artery).
- Clinical Nuance: While considered a gold standard, true “direct” Fick requires a metabolic hood to measure actual VO2. In most cath labs, “indirect” Fick is used, substituting assumed metabolic rates based on age and sex, which introduces error in hypermetabolic or critically ill patients.
B. Indicator Dilution & Thermodilution
A known quantity of an indicator (originally green dye, now cold saline) is injected into the right atrium via a Pulmonary Artery Catheter (PAC). A thermistor at the distal tip measures the temperature drop in the pulmonary artery over time.
- The Formula (Stewart-Hamilton Equation):
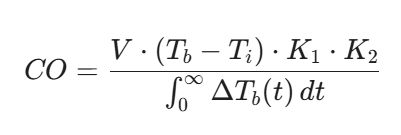
- Where V is injectate volume, Tb and Ti are blood and injectate temperatures, K1, K2 are correction factors, and the denominator is the area under the thermodilution curve.
- Clinical Nuance: Highly accurate but prone to errors in the presence of severe tricuspid regurgitation, intracardiac shunts, or rapid fluid infusions during measurement.
2. Minimally Invasive Methods
A. Pulse Contour Analysis (PiCCO, FloTrac, LiDCO)
These systems utilize algorithms to analyze the arterial pressure waveform morphology obtained from an arterial line. The area under the systolic portion of the curve is proportional to the stroke volume (SV).
- Uncalibrated (e.g., FloTrac/Vigileo): Uses demographic data and waveform characteristics to estimate vascular compliance (C(t)) and resistance.
- Calibrated (e.g., PiCCO, LiDCO): Requires an initial transpulmonary thermodilution or lithium dilution injection to calibrate the vascular compliance factor, offering higher accuracy in unstable shock states.
- Limitations: Highly sensitive to arterial line damping, “whip,” and acute changes in vascular tone (e.g., sudden vasopressor initiation).
B. Esophageal Doppler
A flexible probe is placed in the mid-esophagus to measure blood flow velocity in the descending aorta using the Doppler shift. Stroke volume is calculated by multiplying the velocity-time integral (VTI) by the cross-sectional area of the aorta (derived from nomograms). It provides excellent real-time, beat-to-beat trends but is highly operator-dependent and limited to sedated or intubated patients.
3. Non-Invasive Methods
A. Echocardiography (Doppler Ultrasound)
The clinical workhorse for non-invasive CO measurement. It measures the velocity of blood flow through the Left Ventricular Outflow Tract (LVOT) during systole.
- The Formula:
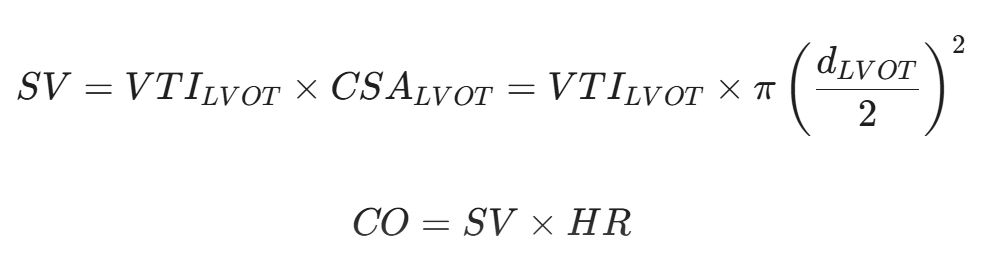
- Where d is the LVOT diameter measured in the parasternal long-axis view, and VTI is traced from the pulse-wave Doppler in the apical 5-chamber view.
- Clinical Nuance: Because the LVOT diameter is squared in the geometric equation, even a 1 mm error in diameter measurement can significantly alter the calculated cardiac output.
B. Bioimpedance and Bioreactance
- Thoracic Electrical Bioimpedance (TEB): Measures changes in electrical resistance across the thorax during the cardiac cycle. As blood (a highly conductive fluid) is ejected into the aorta, resistance decreases.
- Bioreactance (NICOM): An evolution of bioimpedance that measures the phase shift of high-frequency electrical currents as they pass through the thorax. It is less susceptible to motion artifact and patient positioning than older bioimpedance systems.
C. Cardiovascular Magnetic Resonance (CMR)
Utilizes phase-contrast MRI to measure velocity and flow directly within the ascending aorta or main pulmonary artery. It is exceptionally accurate and independent of geometric assumptions, making it the non-invasive gold standard, though limited by cost, availability, and lack of real-time bedside utility.
Modality Comparison Matrix
| Method | Target Parameter | Main Advantage | Primary Limitation |
| Direct Fick | Oxygen consumption / extraction | Gold standard for shunt calculation | Requires invasive arterial/central sampling & true VO2 |
| Thermodilution | Thermal indicator transit | Reliable in stable anatomy; bedside | Blind spot in severe TR or intracardiac shunts |
| Pulse Contour | Arterial pressure wave morphology | Continuous, beat-to-beat tracking | Fails during severe arrhythmias or rapid vasopressor shifts |
| Doppler Echo | LVOT blood velocity profiles | Non-invasive, visualizes structural pathology | Highly operator-dependent; minor geometric errors compound |
| Bioreactance | Thoracic electrical phase shifts | Completely passive, rapid deployment | Less accurate in states of extreme fluid overload/capillary leak |
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal