Inferior wall myocardial infarction
Inferior wall myocardial infarction
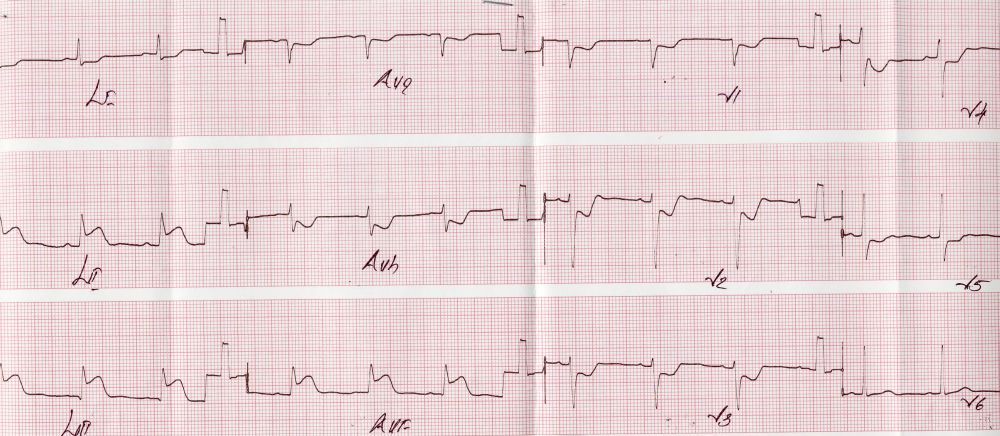
Inferior wall myocardial infarctionECG shows ST segment elevation in leads II, III and aVF of about 3 mm. ST segment depression is seen in leads I, aVl and V1 to V5. Overall features are suggestive of hyperacute phase of inferior wall myocardial infarction with “reciprocal” ST segment depression in anterior leads. The hyperacute phase is diagnosed when the ST segment is elevated and the T waves are upright in those leads. The segment is upsloping in hyperacute phase as the T waves are upright and sometimes a bit tall. ST segment becomes “coved” as the T waves get inverted in the later phase. The “reciprocal” ST depression in anterior leads could be just an electrical phenomenon due to the ST segment elevation in the inferior leads or due to ischemia in the corresponding territory. We will see what exactly was there in this case in the still pictures of left and right coronary angiograms.
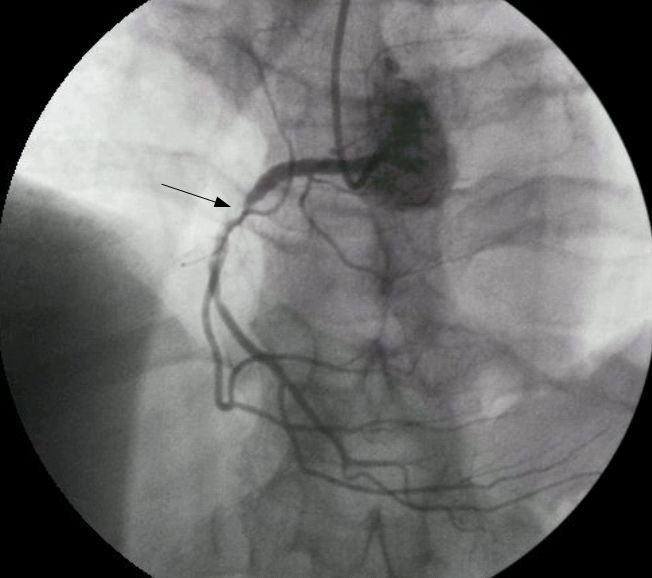
Right coronary angiogram shows a critical lesion with some negative shadows distal to the lesion, suggesting thrombus. Catheter is seen coming from above with no catheter part in the descending aorta near the spine, suggesting that this is possibly a transradial coronary angiogram. We may be tempted to believe that this is the culprit lesion which has caused the inferior wall infarction. Generally the ST elevation is more in lead III in right coronary occlusion while it is more in lead II in left circumflex occlusion. But in this case we have almost equal ST elevation in leads II and III. Let us view the left coronary angiogram and decide.
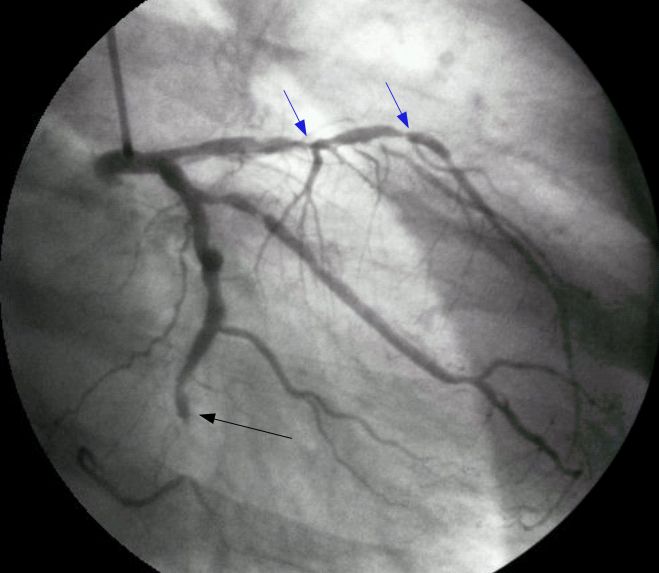
The still picture from left coronary angiogram shows total occlusion of distal left circumflex coronary artery with absent dye filling in a short segment. Multiple significant lesions are seen in left anterior descending coronary artery. Significant lesions are also seen in the obtuse marginal branch of the left circumflex coronary artery. Thus what appeared to be a single vessel disease from the ECG showing hyperacute phase of inferior wall infarction with reciprocal anterior ST segment depression which could occur due to isolated right coronary occlusion, has turned out to be severe triple vessel disease, possibly requiring coronary artery bypass grafting.
The culprit lesion which has caused the infarction in this case is possibly the left circumflex occlusion. When such a set of lesions are seen in the acute phase while taking up the case for primary angioplasty, it is customary to tackle the suspected culprit lesion immediately and consider staged procedure for the remaining lesions. Some operators may consider tackling all lesions if the clinical status permits. But in this case complete revascularization is better done by coronary artery bypass grafting. In this case it was an elective angiogram at a later date and not a pre-primary angioplasty angiogram. So the decision was straightforward, in favour of coronary bypass grafting.
Multi-vessel coronary angioplasty now a days, with the availability of better hardware, especially if the person is not willing for coronary artery bypass grafting.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal