Paced rhythm with very wide QRS
Paced rhythm with very wide QRS
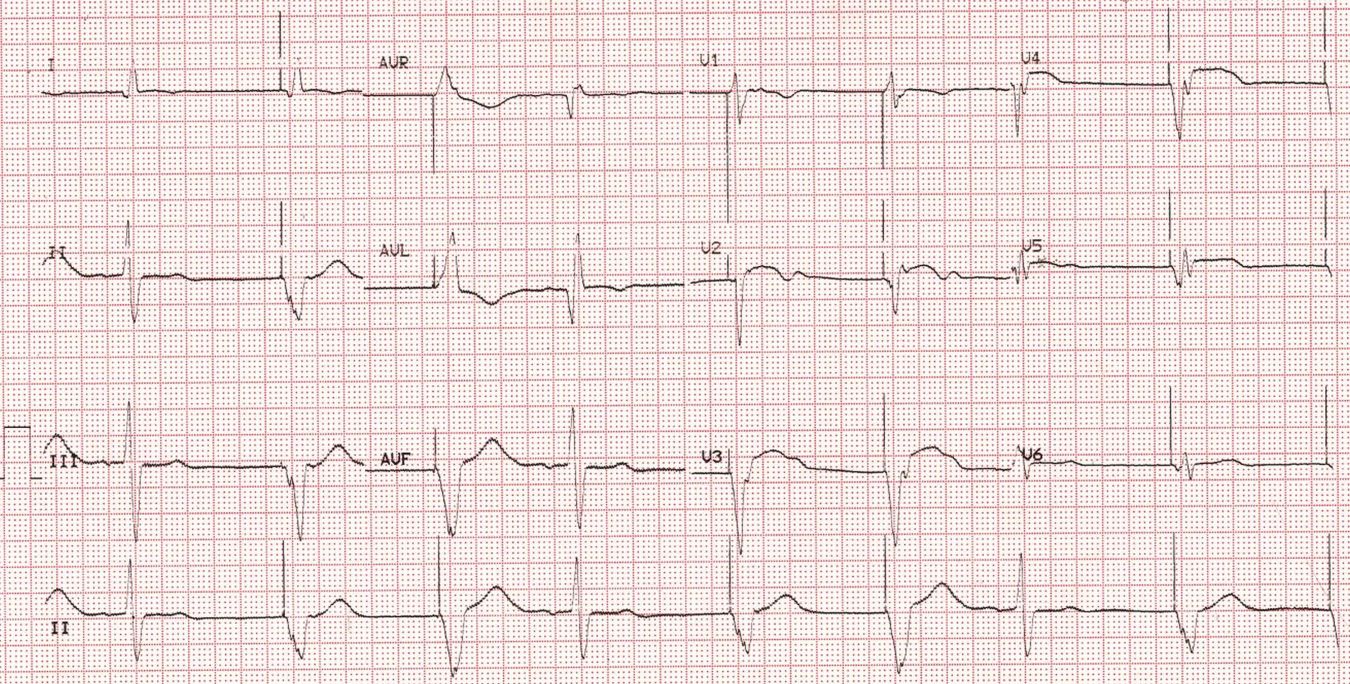
Findings and possible etiology?
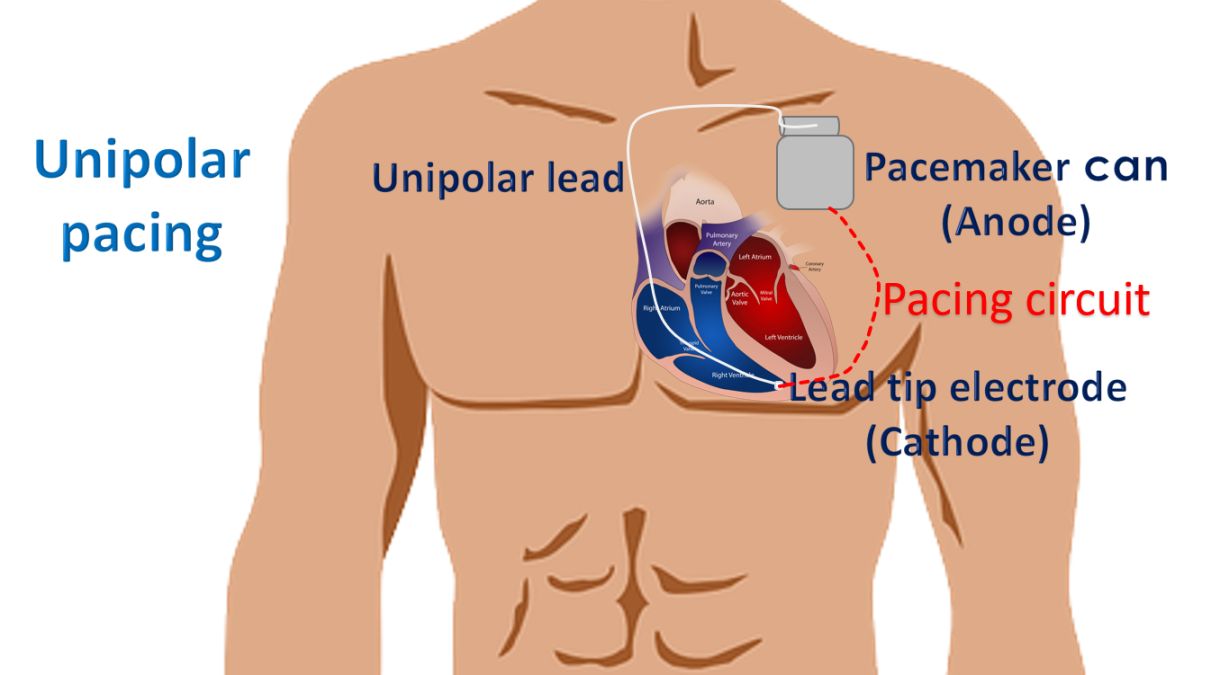
Most of the beats show a large pacing spike just before the QRS complex, indicating a ventricular paced beat, possibly with unipolar pacing mode. In unipolar pacing the lead tip in the right ventricle acts as the negative electrode (cathodal pacing) and the pacemaker can acts as the positive electrode. This causes a long electrical circuit between the two so that surface ECG detects a large pacing spike.
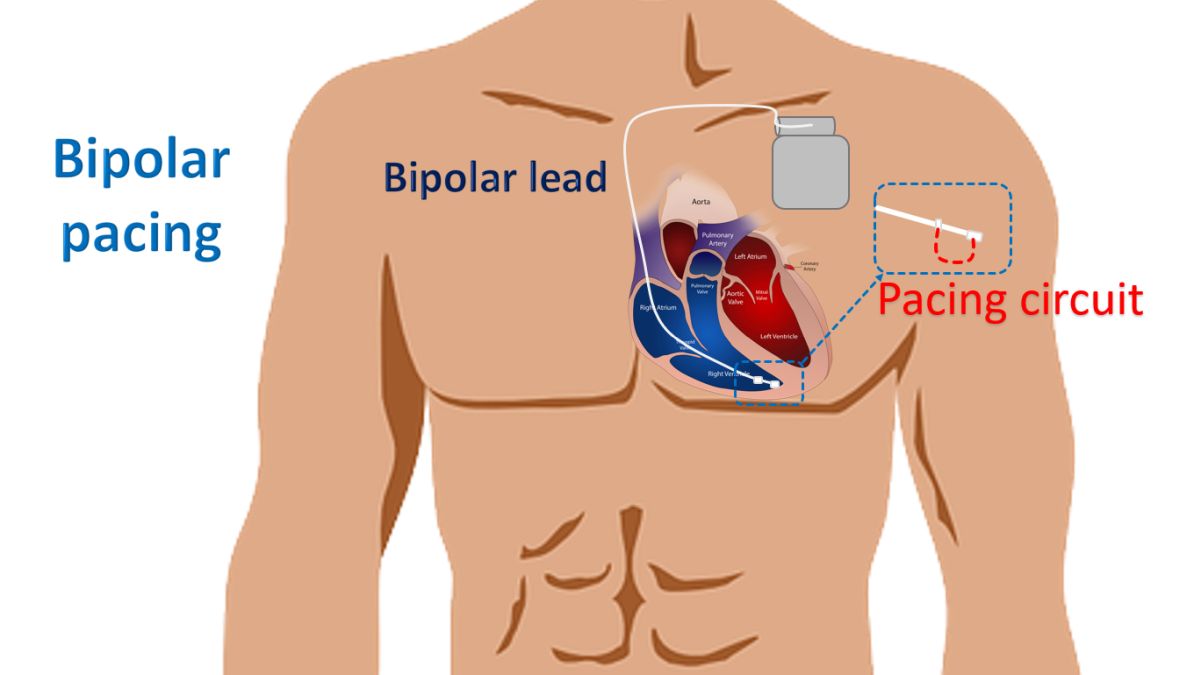
In bipolar pacing, the lead tip is negative, and a proximal ring electrode is positive. So, the pacing circuit is completed within the heart and is very short. Hence the surface ECG detects a small pacing spike.
But in modern day monitors, switching on the pacemaker detection algorithm can also enlarge the displayed spikes. Ventricular rate in this ECG is about 50/min indicating a low programmed pacing rate. Every third complex starting from the first beat seen in the lead II rhythm strip is a spontaneous beat with a PR interval of 160 ms. This would indicate that the indication for pacing would have been sinus node dysfunction as no dissociated P wave are seen. Dissociated P waves would have suggested complete heart block as the reason for ventricular pacing.
QRS complexes have left bundle branch block morphology (negative in V2, V3 and positive in I, aVL). This is seen with right ventricular pacing. Paced complexes are negative in inferior leads. This means that the ventricular activation is proceeding from below upwards, as seen with right ventricular apical pacing.
QR complex with T inversion in the sinus beat in aVL indicates lateral wall infarction. Coved ST segment elevation along with T inversion is seen in paced beats in anterolateral leads, suggesting anterior wall myocardial infarction. The QRS complex of sinus beats show QRS width of 120 ms and left axis deviation suggestive of left anterior hemiblock (LAHB). QRS width of paced beats is 200 ms, indicating significant myocardial damage.
Sgarbossa criteria originally described for diagnosis of myocardial infarction in left bundle branch has been later applied for right ventricular pacing [1].
Reference
- Sgarbossa EB, Pinski SL, Gates KB, Wagner GS. Early electrocardiographic diagnosis of acute myocardial infarction in the presence of ventricular paced rhythm. Am J Cardiol. 1996 Feb 15;77(5):423-4.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal