Intramural VSD
Intramural Ventricular Septal Defect (VSD)
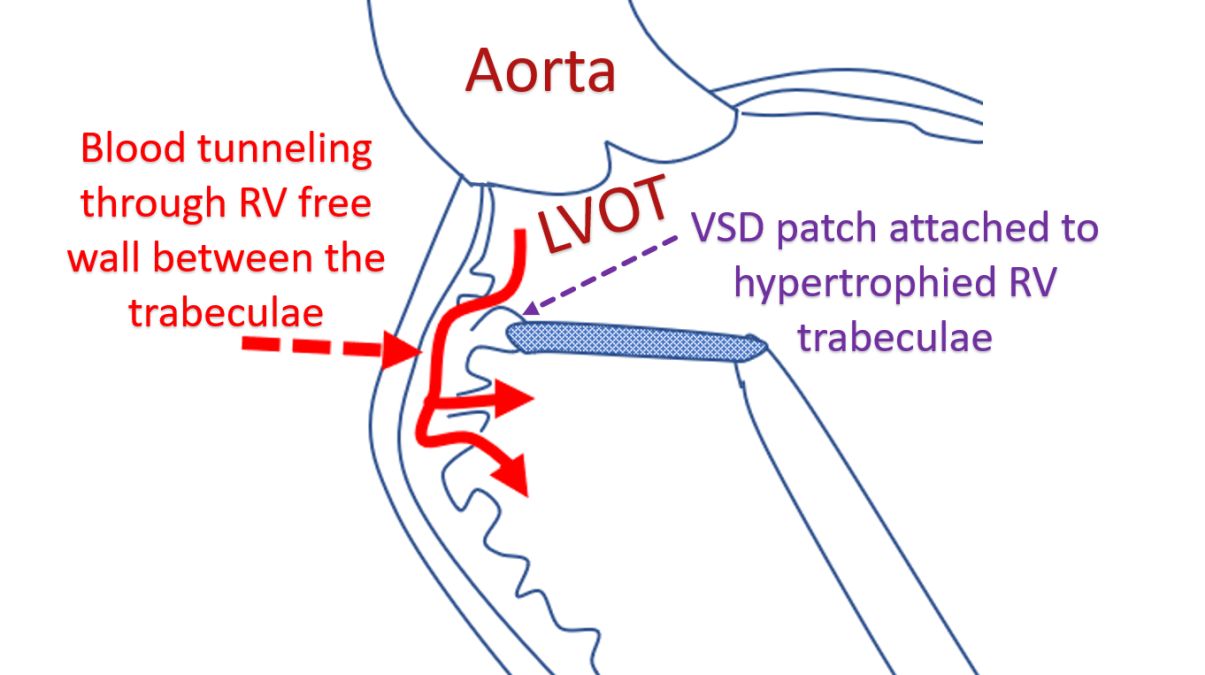
Intramural VSD is a type of residual VSD seen after repair of complex defects like double outlet right ventricle, truncus arteriosus or Rastelli procedure for transposition of great arteries. The intramural VSD originates between the insertion of the VSD closure patch and the aortic valve.
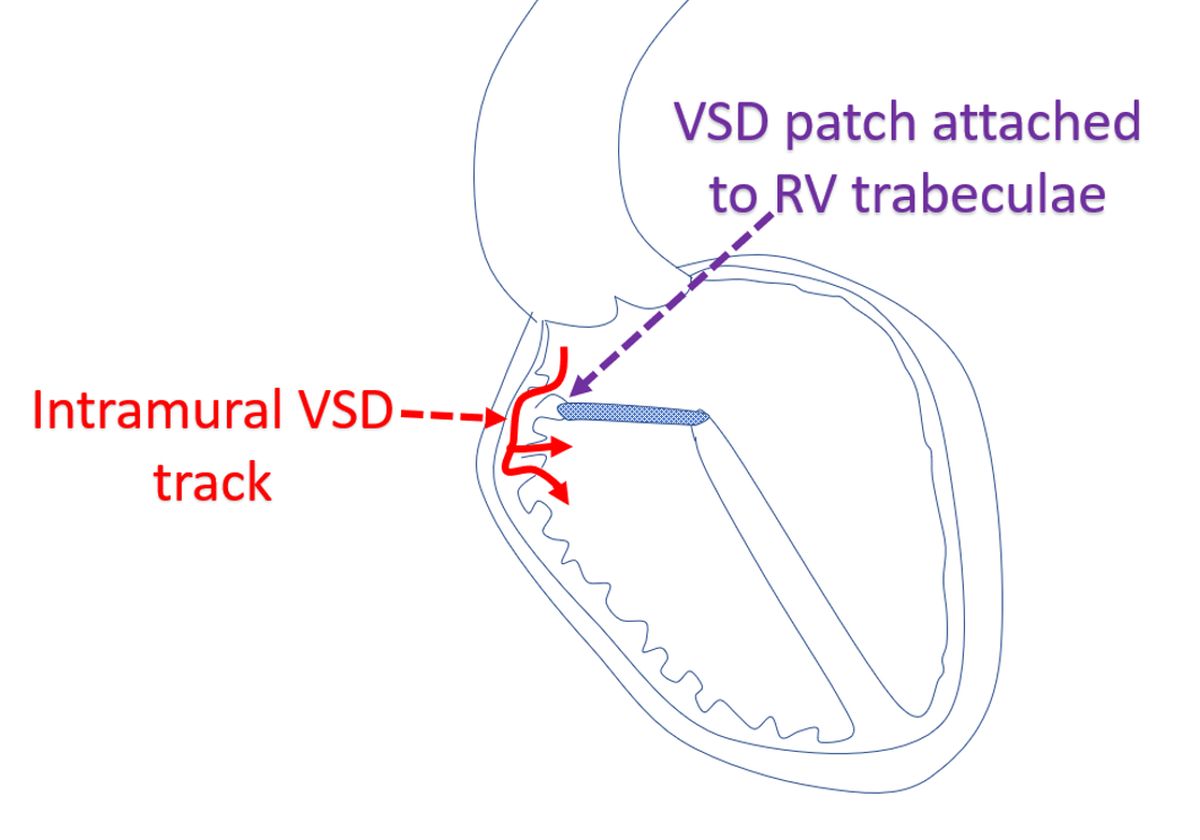
The defect occurs because of coarse trabeculae of the hypertrophic right ventricle prevent good seal at the site of patch insertion so that blood can tunnel through the trabeculae from the left ventricular outflow tract into the right ventricle through its wall (intramural).
Due to the peculiar location, it is often difficult to image intramural VSDs properly, both by transthoracic and transesophageal echocardiography. High parasternal views on trans thoracic and deep trans gastric views on trans esophageal echocardiography are often needed for delineation of the intramural VSDs. The defects can increase in size over time and more shunt can be established.
These shunts may be difficult to eliminate by surgical repair and contribute to morbidity and mortality after the repair of conotruncal anomalies. A study published in Circulation [1] confirmed that intramural VSDs in addition prolong the postoperative hospital stay and need for ECMO (Extracorporeal membrane oxygenator). In their series of 442 subjects, 256 had residual VSDs, of which 49 (11%) were intramural VSDs. Since these VSDs are not accessible through atriotomy or right ventriculotomy, transaortic closure has been advocated [2].
Another study found 34 intramural VSDs in 337 patients who underwent biventricular repair of conotruncal anomalies [3]. 19 were identified both by postoperative transthoracic and intraoperative transesophageal echocardiography. 15 were identified only by postoperative transthoracic echocardiography. Intraoperative transesophageal echocardiography had sensitivity of 56% and specificity of 100% for identifying intramural VSD. Many of the intraoperatively detected defects could be closed fully or partially, but not all.
References
- Patel JK, Glatz AC, Ghosh RM, Jones SM, Natarajan S, Ravishankar C, Mascio CE, Spray TL, Cohen MS. Intramural Ventricular Septal Defect is a Distinct Clinical Entity Associated with Postoperative Morbidity in Children after Repair of Conotruncal Anomalies. Circulation. 2015; 132: 1387-1394.
- Belli E, Houyel L, Serraf A, Lacour-Gayet F, Petit J, Planché C. Transaortic closure of residual intramural ventricular septal defect. Ann Thorac Surg. 2000 May;69(5):1496-8.
- Patel JK, Glatz AC, Ghosh RM, Jones SM, Ravishankar C, Mascio C, Cohen MS. Accuracy of transesophageal echocardiography in the identification of postoperative intramural ventricular septal defects. J Thorac Cardiovasc Surg. 2016 Sep;152(3):688-95.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal