Invasive blood pressure monitoring
Invasive blood pressure monitoring
Illustrated notes
 Invasive blood pressure monitoring is fairly common in the acute care setting. A small cannula is introduced percutaneously into the radial artery or any other artery which is easily accessible and the proximal end connected to the pressure transducer through a three way stop cock system. A high pressure drip attached to one port of the three way system allows continuous flushing of the system at a slow rate of around 3 ml per hour.
Invasive blood pressure monitoring is fairly common in the acute care setting. A small cannula is introduced percutaneously into the radial artery or any other artery which is easily accessible and the proximal end connected to the pressure transducer through a three way stop cock system. A high pressure drip attached to one port of the three way system allows continuous flushing of the system at a slow rate of around 3 ml per hour.
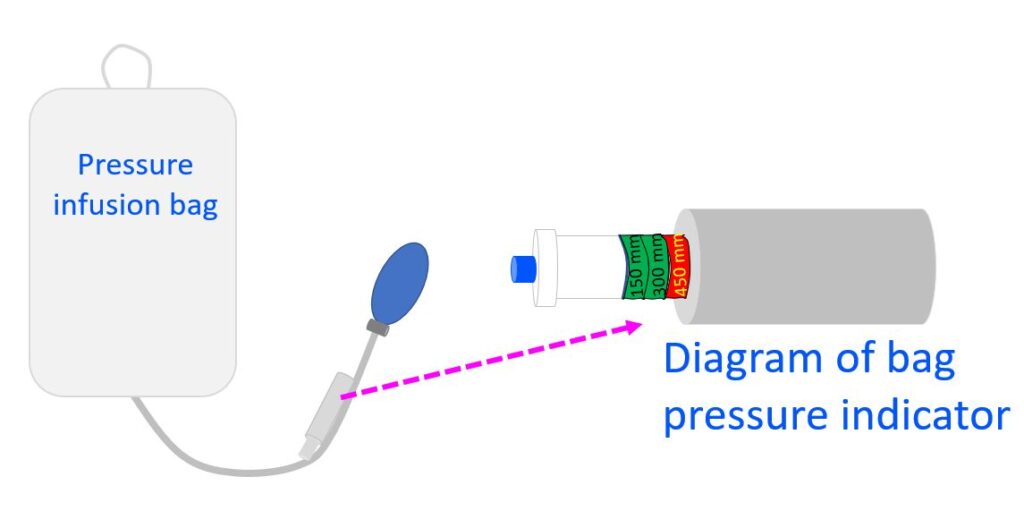
The fluid to be used for flushing is kept in a sterile collapsible bag and the bag is encased by a pressure delivery system or pressure infusion bag. The pressure within the enclosure can be raised to 300 mm Hg and is demonstrated by the indicator piston progressively coming out with initial marking at 150 mm Hg and the next marking at 300 mm Hg. Both these marks are coloured green while beyond this level the markings are in red and in some systems there is provision for automatic deflation to lower levels when the pressure is raised beyond the permissible level.
Pressure within the bag is raised using a mechanism similar to the bellows of the sphygmomanometer. There is a flushing valve for the transducer assembly which can be used to flush the cannula with higher flow rate if needed, to relieve any partial obstruction due to clot formation. When a small handle of the flushing port is pulled out the drip flows fast as the whole 300 mmHg compression force is freely delivered to the infusion system. Small amount of heparin is added to the flush solution, usually normal saline, to prevent clot formation at the tip of the cannula within the artery.
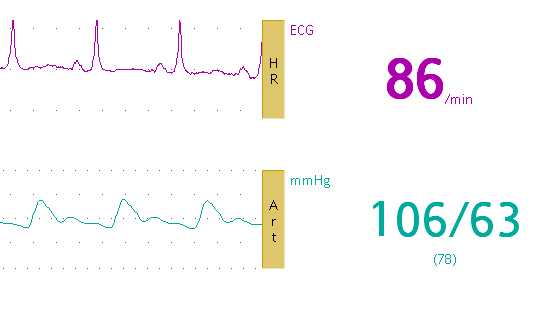
Invasive monitors usually display ECG, pulse oximetry tracing and respiration along with the invasive blood pressure. End tidal carbon dioxide or ETCO2 module can also be incorporated when needed, mostly in patients on intermittent positive pressure ventilation.
In the picture shown here, the violet tracing represents the ECG and green tracing the invasive intra arterial blood pressure. The heart rate is displayed as 86 per minute and blood pressure as 106/63 mm Hg with a mean arterial pressure of 78 mm Hg. Very often in the critical care setting the intensivists depend on mean arterial pressure to titrate the dose of pressor agents while treating shock.
If the invasive arterial tracing does not show a good wave form, the cannula has to be flushed. If still the pressure tracing is not good, it may be worthwhile changing the site of the arterial cannula.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal