LBBB with First Degree AV Block
LBBB with First Degree AV Block
Left bundle branch block (LBBB) with first degree AV Block is a type of trifascicular block, since the PR interval prolongation could indicate that the conduction in the right bundle is also affected. LBBB with first degree AV block has also been called bilateral bundle branch block [1].
LBBB with first degree AV block could also be due to a co-existent conduction delay in the AV node, rather than in the infra Hisian conduction system. In a study of 12 patients by Rosen KM et al, 6 patients developed type I second degree AV block on atrial pacing, with location proximal to His bundle [2]. Two patients developed type II AV block with location distal to the bundle of His. Other patients had both type I and type II responses.
Transient syncope and LBBB with first degree AV block has been reported in a patient after taking Propafenone as ‘pill in the pocket’ for paroxysmal atrial fibrillation and supraventricular tachycardia [3]. The patient was also on carvedilol for hypertension. ECG changes reverted during observation.
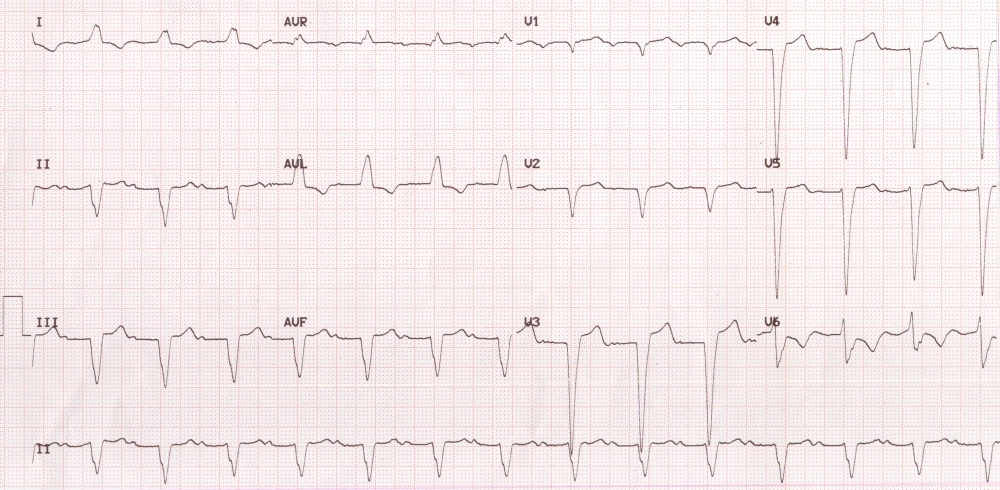
LBBB with first degree AV block may be considered as a forerunner of complete AV block. First degree AV block in this ECG is manifest as the prolonged PR interval of 280 milliseconds. LBBB is manifest as broad notched QRS complexes in lead I and aVL. The poor progression of R waves and wide QS complexes in anterior leads are also consistent with LBBB. But V6 is not showing a wide notched predominantly positive QRS complex. This disparity between V6 and lead I are often seen when the QRS axis is leftward in LBBB. Inferior and anterior leads are showing a pseudo infarction pattern, which is common with LBBB.
QRS duration of more than 120 milliseconds with LBBB pattern in a person with refractory heart failure will be an indication for cardiac resynchronization therapy (CRT, biventricular pacing, heart failure device). It is often associated with mechanical dyssynchrony and wasted systolic effort of the left ventricle. CRT produces a narrowing of the QRS complexes as the right ventricle and posterolateral left ventricle are paced in synchrony, to produce a better left ventricular output.
References
- Schloff LD, Adler L, Donoso E, Friedberg CK. Bilateral bundle-branch block. Clinical and electrocardiographic aspects. Circulation. 1967 Apr;35(4):790-801.
- Rosen KM, Rahimtoola SH, Chuquimia R, Loeb HS, Gunnar RM. Electrophysiological significance of first degree atrioventricular block with intraventricular conduction disturbance. Circulation. 1971 Apr;43(4):491-502.
- Patanè S, Marte F, Di Bella G. Transient syncope, left bundle branch block and first degree atrioventricular block after “pill-in-the-pocket” administration. Int J Cardiol. 2008 May 7;126(1):e19-21.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
In this case would it be incorrect to read the ECG as Sinus rhythm with first degree AV block, LBBB? should the reading be sinus rhythm with prolonged PR, LBBB? Thanks!
Of this patient needs elective surgery, is it necessary to have him reviewed by cardiologist and ICD insertion preoperatively.
A person with similar ECG will benefit from preoperative cardiac evaluation. Decision regarding implantation of ICD needs further clinical work up to see if criteria for implantation of an ICD are satisfied.