Left internal mammary artery (LIMA) angiogram
Left internal mammary artery (LIMA) angiogram
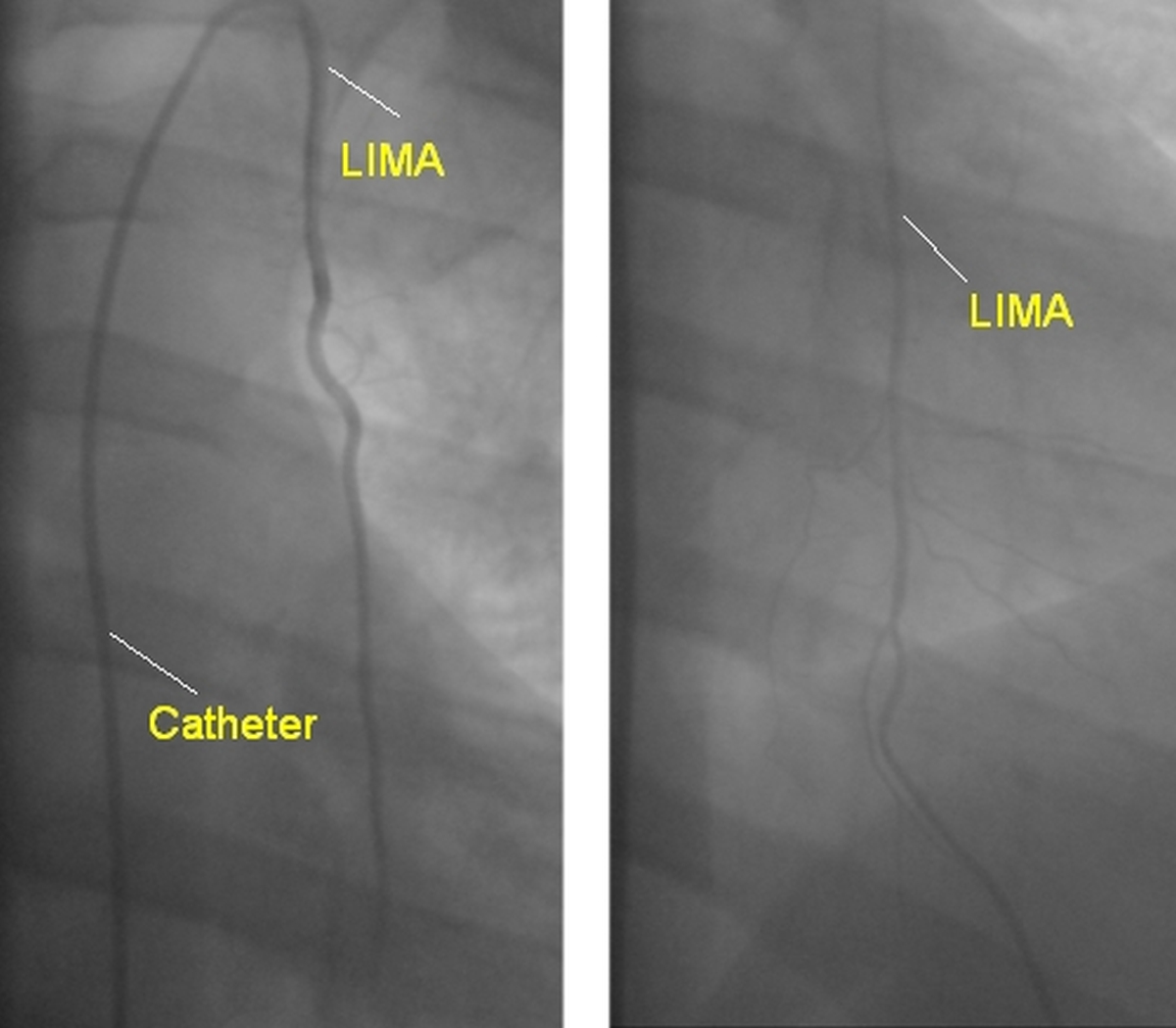
Left internal mammary artery can be cannulated by access through the left subclavian artery. Selective cannulation is not essential for visualising the LIMA. The left frame shows the initial portion of the artery while the second frame shows the artery branching into superior epigastric and musculophrenic arteries.
The musculophrenic artery supplies the diaphragm and the superior epigastric artery tracks down and anastomoses with branches of the inferior epigastric arteries. This anastomosis becomes prominent in aortic obstructions below the level of the left subclavian artery and can be demonstrated angiographically.
It is easier to directly cannulate the internal mammary artery by the trans femoral arterial approach. Most often the right Judkins coronary catheter is used for LIMA angiography. Occasionally a special LIMA catheter may be used. LIMA angiography is done when a coronary artery bypass graft surgery to the left anterior descending coronary artery is being considered.
It is also done for the evaluation of post CABG patients who develop angina pectoris. As mentioned earlier, it is rarely done to demonstrate the collaterals in case of aortic obstruction. While approaching from the transradial route using a Tiger catheter, selective entry into the LIMA is often difficult and a left subclavian angiogram is done instead.
Left subclavian angiogram also demonstrates the LIMA well. This is most often sufficient and a selective cannulation is avoided. Compression of left brachial artery during injection into the left subclavian reduces the runoff into the left upper limb and increases the opacification of the LIMA. This can be done either manually or using the cuff of a blood pressure apparatus.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal