MAPCA from right internal mammary artery (RIMA)
MAPCA from right internal mammary artery (RIMA)
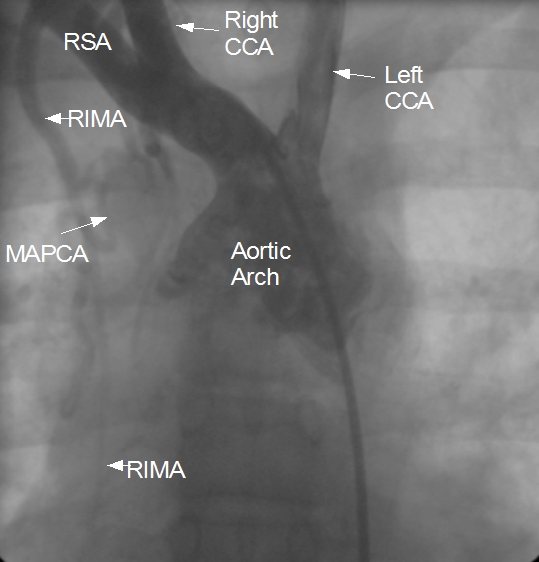
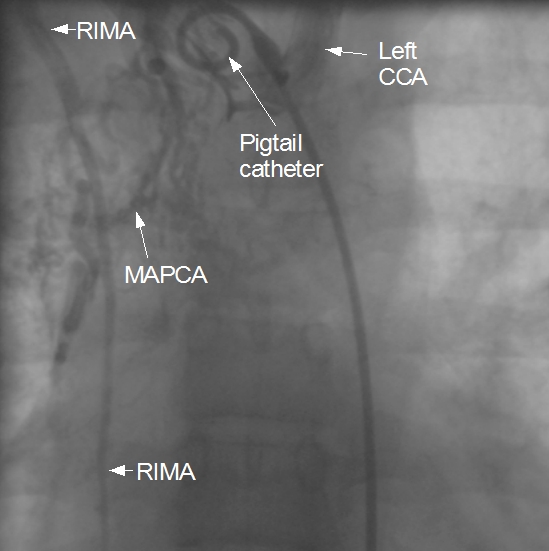
Still frame from an angiogram with radiocontrast dye injected using a pigtail catheter kept in the right brachiocephalic artery showing major aortopulmonary collateral artery (MAPCA) arising from the right internal mammary artery (RIMA). RSA: right subclavian artery; Right CCA: right common carotid artery; Left CCA: left common carotid artery. Left subclavian artery is not visualised well as the dye reflux into the arch of aorta is not enough to opacify it and the proximal holes of the pigtail are beyond its origin. The second frame (below) gives a better picture of the tortuous branches of the MAPCA. MAPCAs are seen in severe forms of Tetralogy of Fallot and pulmonary atresia. MAPCAs can originate from either of the subclavian arteries or their branches, transverse aorta, descending thoracic aorta, abdominal aorta at or below the level of the diaphragm or coronary artery [1].
When the lungs are supplied by multiple MAPCAs, they are unifocalised prior to definitive surgical repair of Tetralogy of Fallot. Connecting the distal end of MAPCAs to a single vessel is known as unifocalization. Collaterals to the pulmonary arterial branches can also arise from the bronchial arteries within the lungs. Hilar collaterals can also occur in pulmonary atresia.
Reference
- Adamson GT, McElhinney DB, Zhang Y, Feinstein JA, Peng LF, Ma M, Algaze CA, Hanley FL, Perry SB. Angiographic Anatomy of Major Aortopulmonary Collateral Arteries and Association With Early Surgical Outcomes in Tetralogy of Fallot. J Am Heart Assoc. 2020 Dec 15;9(24):e017981.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal