Mechanisms of aortic regurgitation in aortic dissection
Mechanisms of aortic regurgitation in aortic dissection
Aortic regurgitation is the second most common cause of death in acute aortic dissection, most common cause being aortic rupture. It may occur in up to three fourths of cases of Stanford Type A aortic dissection.
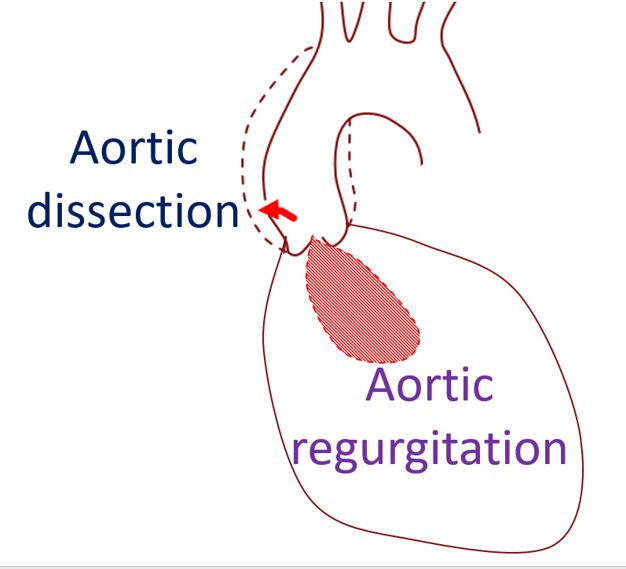
There are several mechanisms for aortic regurgitation in aortic dissection:
- Dilatation of the aortic root and annulus
- Tearing of aortic annulus or cusps of the aortic valve
- Displacement of aortic cusps in relation to each other, interfering with closure
- Loss of support for aortic cusps
- Intimal flap interfering with closure of aortic cusps
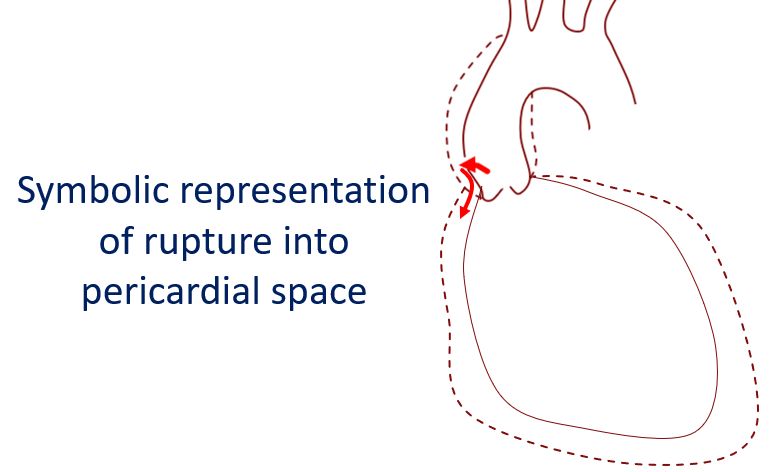
Those with severe aortic regurgitation secondary to acute aortic dissection present with acute left ventricular failure and cardiogenic shock. Pericardial tamponade may also be associated if the dissection ruptures into the pericardial sac.
In one study, there were 16 with intrinsically normal leaflets with aortic regurgitation due to correctable lesions: Incomplete leaflet closure due to aortic leaflet tethering in a dilated aortic root in 7, prolapse of leaflet due to disrupted attachment in 8 and prolapse of dissection flap through the aortic valve orifice in 5 [1]. These defects were identified pre-operatively by transesophageal echocardiography. Of this 16, successful aortic valve repair was achieved in 15 while one needed aortic replacement after a complicated intraoperative course unrelated to the aortic valve.
Reference
- Movsowitz HD, Levine RA, Hilgenberg AD, Isselbacher EM. Transesophageal echocardiographic description of the mechanisms of aortic regurgitation in acute type A aortic dissection: implications for aortic valve repair. J Am Coll Cardiol. 2000 Sep;36(3):884-90.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal