Mild tricuspid regurgitation and borderline pulmonary arterial hypertension – Echocardiogram video
Mild tricuspid regurgitation and borderline pulmonary arterial hypertension – Echocardiogram video
Echocardiogram video with narration
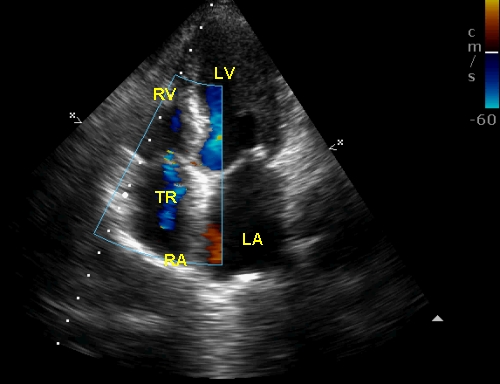
Apical four chamber view with colour flow mapping demonstrates mild tricuspid regurgitation (TR) as a bluish mosaic jet into the right atrium. RA: right atrium; LA: left atrium; LV: left ventricle; LA: left atrium. Both mitral and tricuspid valves are in closed position, indicating a systolic frame. TR jet area occupies only a small portion of the right atrial area, qualifying for mild tricuspid regurgitation. Interventricular septum (between RV and LV) atrioventricular septum (between the septal attachments of the mitral and tricuspid valves) and the interatrial septum (between RA and LA) are clearly seen in this view.
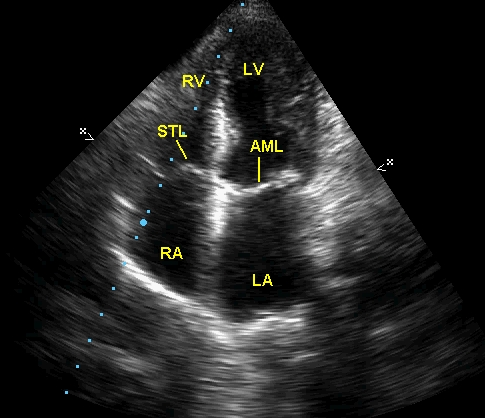
Apical four chamber view without color flow mapping. STL: septal tricuspid leaflet; AML: anterior mitral leaflet. The region of the septum between the STL and AML is the atrioventricular septum. If there is a defect in this region of the septum it will cause and LV-RA shunt and it is called Gerbode VSD (ventricular septal defect). If the STL is attached far distally, then it is called Ebstein’s anomaly of the tricuspid valve, in which a portion of the right ventricle becomes atrialised.
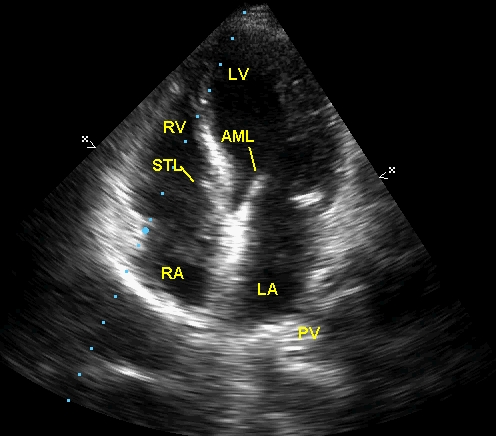
Apical four chamber view with mitral and tricuspid valves partially open. The STL and AML are seen well and valve openings are good. PV: pulmonary vein, draining to the left atrium. Note that the ventricular cavities are larger in the diastolic frame.
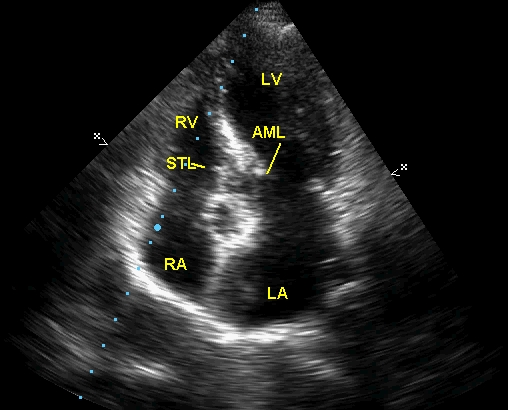
Apical four chamber view showing fully open mitral and tricuspid valves. It can be seen that both AML and STL are flush with the interventricular septum and barely discernible as separate structures in this view. The view gets slightly tilted due to the cardiac motion so that aorta gets opened up partially, though it is not a typical five chamber view.
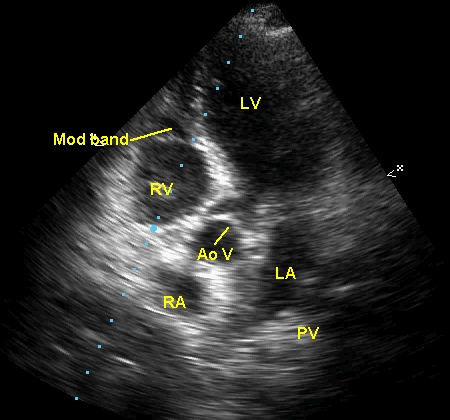
Apical five chamber view showing the aortic valve (Ao V) and the moderator band (Mod band). Right bundle branch traverses through the region of the moderator band. The five chamber view (5C view) is obtained by tilting the transducer while in the four chamber view in such a way that the beam is directed a little more anteriorly.
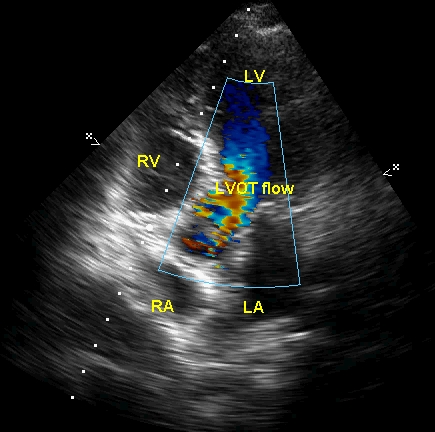
Apical five chamber view (5C) view with color flow mapping (CFM) showing the blue coloured flow from the left ventricle converging to the left ventricular outflow tract (LVOT). There is some turbulence in the LVOT, which could be due to narrowing of the LVOT, hyperdynamic circulation or due to the lower Nyquist limit which has been set.
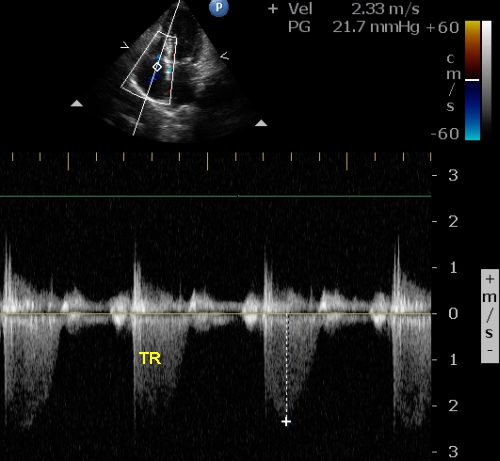
Apical four chamber view is seen in the upper panel, used for guiding the Doppler line for interrogating the region of the tricuspid valve to get the tricuspid regurgitation (TR) jet in lower panel. The peak velocity has been measured and displayed at the top as 2.33 m/s. The calculated gradient has also been displayed: 21.7 mm Hg. The Nyquist limit of the color Doppler system has been displayed near the color bar as 60 cm/s. The TR jet envelope is incomplete in most cycles, indicating that it is a mild TR. Calculated right ventricular systolic pressure (RVSP) is 31.7 mm Hg, assuming a right atrial pressure of 10 mm Hg, indicating mild (borderline) pulmonary hypertension. Systolic pressure above 30 mm Hg and mean pressure above 20 mm Hg in the pulmonary artery is usually taken as elevated.
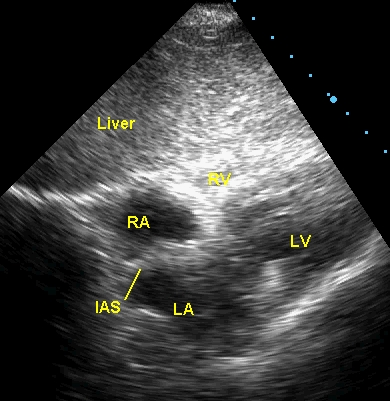
Subcostal view demonstrating the interatrial septum (IAS) and the liver above the heart. This is a good view for imaging the interatrial septum as false drop outs are unlikely as the IAS is perpendicular to the imaging ultrasound beam in this view. The Doppler flow can also be detected well as it will be parallel to the beam. The only disadvantage in an adult is the possibility of poor images when the costal angle is narrow in lean individuals and difficulty in getting a good view in those with abdominal obesity.
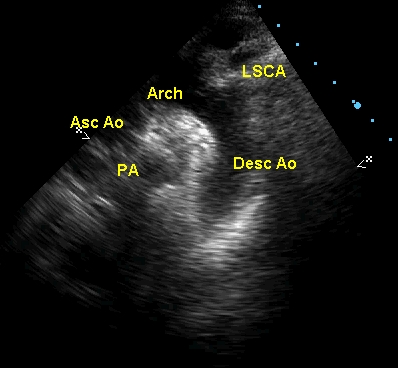
Supra sternal view showing the ascending aorta (Asc Ao), arch of aorta (Arch), descending aorta (Desc Ao), pulmonary artery (PA) and left subclavian artery (LSCA). This is a good view to image coarctation of aorta, especially the post subclavian variety, which can be seen as a shelf like structure just below the left subclavian artery.
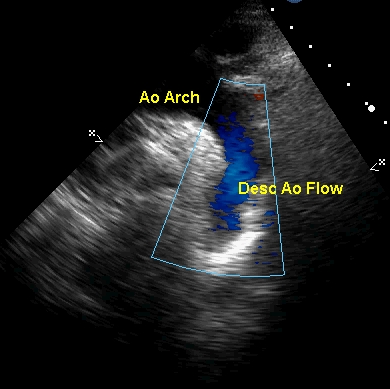
Supra sternal view with colour flow mapping demonstrating the blue colored flow in descending aorta. When there is a persistent left superior vena cava, it can be imaged in this view, with blue coloured flow, lateral to the descending aorta. A vertical vein either partial or total anomalous pulmonary venous connection can also be imaged in this view. In that case the flow will be upwards and detected as a red coloured flow.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal