Mural endocarditis
Mural endocarditis
Vegetations in infective endocarditis are usually situated on the valves. If they are located on the walls of the cardiac chambers, it is known as mural endocarditis [1]. When mural endocarditis occurs without any cardiac structural abnormalities like ventricular septal defects, it is called primary mural endocarditis [2]. Primary mural endocarditis is extremely rare.
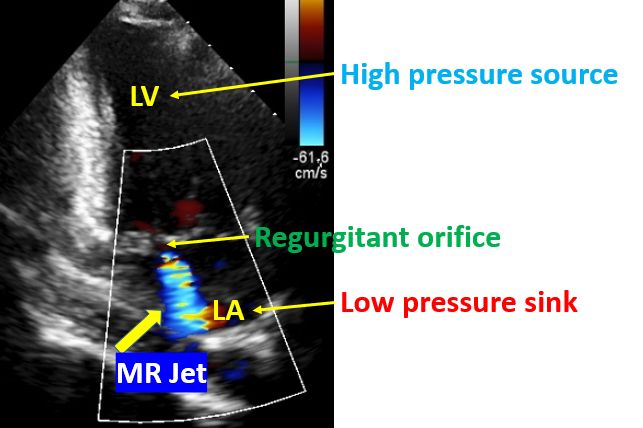
Left atrial mural endocarditis usually occurs due to the jet lesion of mitral regurgitation [1,3]. Left atrial mural endocarditis is usually picked up by trans esophageal echocardiography. Vegetations are mostly located just distal to the mitral orifice between the high pressure jet and a low pressure sink. This concept was well explained by Rodbard in 1963 [4]. He noted that endocarditis occurs when a high pressure source extrudes blood at critical velocities through a narrow orifice into a low pressure sink. The following picture illustrates this concept.
High velocity jets of mitral or aortic regurgitation on the cardiac chamber wall produces endothelial denudation. Platelets and fibrin get deposited on these jet lesions and serves as a nidus for endocarditis during transient bacteremia. It has been suggested that when surgical treatment is planned for endocarditis, complete removal of these lesions is necessary to clear bacteremia, decrease embolic complications and prevent relapse after completion of antibiotic therapy [5].
Jet lesions will be in the right ventricle in ventricular septal defect, while it can be in the left ventricle in aortic regurgitation. In case of aortic stenosis and coarctation of aorta, it will be in the aorta. Patent ductus arteriosus produces jet lesion in the pulmonary artery. So the location of mural endocarditis will be in these locations in those conditions.
Risk factors for primary mural endocarditis include immunosuppression, intravenous drug abuse, prior cardiac surgery and chronic debilitating disease [6]. Most common etiological agents in mural endocarditis are Staphylococcus aureus and Streptococcus species.
GAMES registry involving 35 Spanish hospitals documented 27 cases of mural endocarditis among 3676 cases of infective endocarditis between 2008 and 2017 [7]. Patients with mural endocarditis were younger with a median age of 59 years in that registry. Transplantation, hemodialysis, catheter source and Candida etiology were more common in the mural endocarditis group. Mortality was similar between the groups. But Charlson Index was lower (4 versus 5 ) in the mural endocarditis group.
In most cases of isolated left atrial mural endocarditis, the mitral regurgitation jet is eccentric and directed towards left atrial wall. In most cases mitral regurgitation was relatively mild and vegetation was located at the posterior wall, which was just above the mitral valve and exposed to the regurgitant jet [1].
References
- Hosokawa S, Okayama H, Hiasa G, Kawamura G, Shigematsu T, Takahashi T, Kawada Y, Yamada T, Matsuoka H, Kazatani Y. Isolated Left Atrial Infective Mural Endocarditis. Intern Med. 2018 Apr 1;57(7):957-960. doi: 10.2169/internalmedicine.9559-17. Epub 2017 Dec 8. PMID: 29225261; PMCID: PMC5919852.
- Tahara M, Nagai T, Takase Y, Takiguchi S, Tanaka Y, Kunihara T, Arakawa J, Nakaya K, Hamabe A, Gatate Y, Kujiraoka T, Tabata H, Katsushika S. Primary Mural Endocarditis Without Valvular Involvement. J Ultrasound Med. 2017 Mar;36(3):659-664. doi: 10.7863/ultra.16.03049. Epub 2017 Jan 27. PMID: 28127793.
- Reddy G, Chatterjee A, Leon K. Left atrial mural endocarditis secondary to mitral valve jet lesion. Circulation. 2015 Apr 28;131(17):1529-30. doi: 10.1161/CIRCULATIONAHA.115.015626. PMID: 25918043.
- Rodbard S. Blood velocity and endocarditis. Circulation. 1963 Jan;27:18-28. doi: 10.1161/01.cir.27.1.18. PMID: 13974594.
- Reddy G, Chatterjee A, Leon K. Left atrial mural endocarditis secondary to mitral valve jet lesion. Circulation. 2015 Apr 28;131(17):1529-30. doi: 10.1161/CIRCULATIONAHA.115.015626. PMID: 25918043.
- Hussain U, Abdulrazzaq M, Goyal A. Primary Mural Endocarditis Caused by Streptococcus pyogenes. CASE (Phila). 2019 Oct 16;3(6):259-262. doi: 10.1016/j.case.2019.09.001. PMID: 32002480; PMCID: PMC6985001.
- Gutiérrez-Villanueva A, Muñoz P, Delgado-Montero A, Olmedo-Samperio M, de Alarcón A, Gutiérrez-Carretero E, Zarauza J, García I Pares D, Goenaga MÁ, Ojeda-Burgos G, Goikoetxea-Agirre AJ, Reguera-Iglesias JM, Ramos A, Fernández-Cruz A; Spanish Collaboration on Endocarditis—Grupo de Apoyo al Manejo de la Endocarditis infecciosa en España (GAMES). Mural Endocarditis: The GAMES Registry Series and Review of the Literature. Infect Dis Ther. 2021 Jul 26. doi: 10.1007/s40121-021-00490-y. Epub ahead of print. PMID: 34312819.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal