Renal Angiography and Angioplasty
Renal angiography and angioplasty
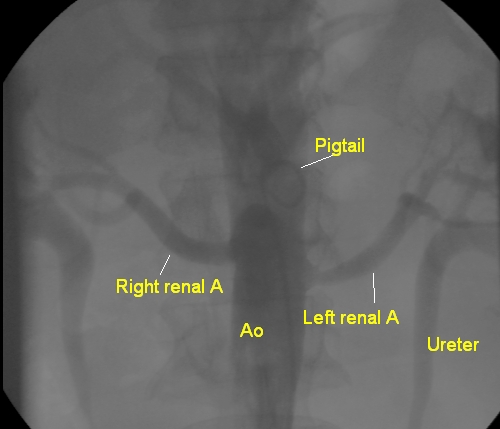
Here is a descending aortogram with pigtail catheter showing both renal arteries arising from the aorta. Left renal artery shows narrowing in the proximal segment just after the ostium. Selective renal angiograms can be obtained by introducing either a Judkins right coronary catheter or a cobra catheter into the renal artery ostium and gently injecting contrast to fill the renal arteries. The imaging is continued till the nephrogram phase is obtained. It may be better to do selective angiograms after locating the renal arteries by non-selective aortograms as in this case. This will help to identify multiple renal arteries if present. If multiple renal arteries are present and stenotic, the option may be in favour of surgical correction rather than catheter based intervention.
Renal angioplasty
Once the renal arterial anatomy has been documented, one may proceed with interventions if the stenosis is severe and angioplasty indicated. In general renal angioplasty is considered only for lesions which produce uncontrolled hypertension or deterioration of renal function. Angioplasty is seldom done for lesions incidentally detected during angiography for atherosclerotic lesions elsewhere. Recurrent flash pulmonary edema known as Pickering syndrome [1], is an important indication for renal angioplasty. The reason for restrictive use of angioplasty is the lack of evidence regarding benefit from angioplasty of incidentally detected renal artery stenosis.
Specific renal guide catheters are available for use during renal angioplasty. Alternatively, Judkins right coronary guide can also be used. Approach is often through the femoral arterial puncture, while occasional caudally directed renal arteries may be better approached through the brachial route. Guide wire used could be 0.014″ coronary guide wire or the 0.035″ guide wire depending on the compatibility of the balloon system to be used. Hydrophilic wires are better avoided, though they may have to be used sometimes. The wire tip is parked as distally as feasible to get a good support. Distal protection devices are seldom used for renal angioplasty. The evidence favouring them is not definite and hence they are not currently recommended. Often there is no good landing zone for the distal protection device due to early branching of the renal artery.
Once the guide is stabilized in the ostium and a guide wire positioned across the lesion, a predilatation balloon is introduced across the lesion and inflated. Check angiogram is obtained to confirm opening up of the lesion and excluding dissection. An adequate sized balloon mounted stent is then introduced over the guide wire after removing the predilatation balloon. The stent is positioned and accuracy of position checked with short puffs of dye in multiple angiographic projections. The stent balloon is then inflated, often beyond the nominal values, to get good apposition of the stent with full expansion. Patient can experience mild abdominal pain during the inflation. Check angiograms are obtained to see the result.
Hypertension may persist despite successful renal angioplasty. A deterioration of renal function in some cases may also be anticipated due to atheroembolism. But good recovery can be expected in most cases. Use of contrast has to be minimised to reduce the chance for contrast nephropathy. Tackling both sides in the same sitting also increases the chance of deterioration of renal function.
Reference
- Shrimal P, Sahu AK, Mathew R, Bansal A. Pickering syndrome: a rare presentation in emergency department. BMJ Case Rep. 2021 Feb 9;14(2):e239421. doi: 10.1136/bcr-2020-239421. PMID: 33563668; PMCID: PMC7875303.
Related Posts
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal