Risk stratification for SCD in CHD focusing on TOF
Risk stratification for SCD in CHD focusing on TOF
Risk stratification for SCD in CHD focusing on TOF: Sudden cardiac death (SCD) in tetralogy of Fallot (TOF) is the most well studied. Taussig’s group was one of the earliest to report post repair SCD in TOF. Right bundle branch block (RBBB) is thought to be a risk factor. QRS duration >180 ms was found to be correlated with SCD. RBBB also correlates with larger right ventricular size.
A study of 178 adult survivors of tetralogy of Fallot repair with mean follow up of 21.4 years had 9 patients with sustained ventricular tachycardia [1]. Eight had near miss sudden death. There were an additional 4 post operative sudden deaths. Of the 178 patients, 41 with mean follow up of 23.6 years were prospectively studied with 12 lead ECG, chest X-ray and echocardiography. QRS duration in these patients ranged from 90 to 200 ms and correlated with cardiothoracic ratio on chest X-ray and right ventricular size on echocardiography. The 9 patients with ventricular tachycardia had QRS duration between 180 – 230 ms and cardiothoracic ratio ranged from 0.54 to 0.9. All patients with ventricular tachycardia and the 4 patients with sudden death had QRS duration above 180 ms.
Another study retrospectively evaluated 89 patients who had undergone total repair of TOF and followed up for more than 10 years [2]. One patient died of cerebral bleeding and two had sudden cardiac death. Overall survival at 20 years was 100% and that at 40 years was 94.6%. Eight patients required late reinterventions. Four were for right ventricular outflow, 2 for aortic valve and 2 others. Ten patients had ventricular tachycardia or fibrillation and six underwent implantation of an implantable cardioverter defibrillator. On multivariate analysis, rapid change of QRS duration and higher tricuspid regurgitation gradient were risk factors for ventricular tachyarrhythmia late after TOF repair.
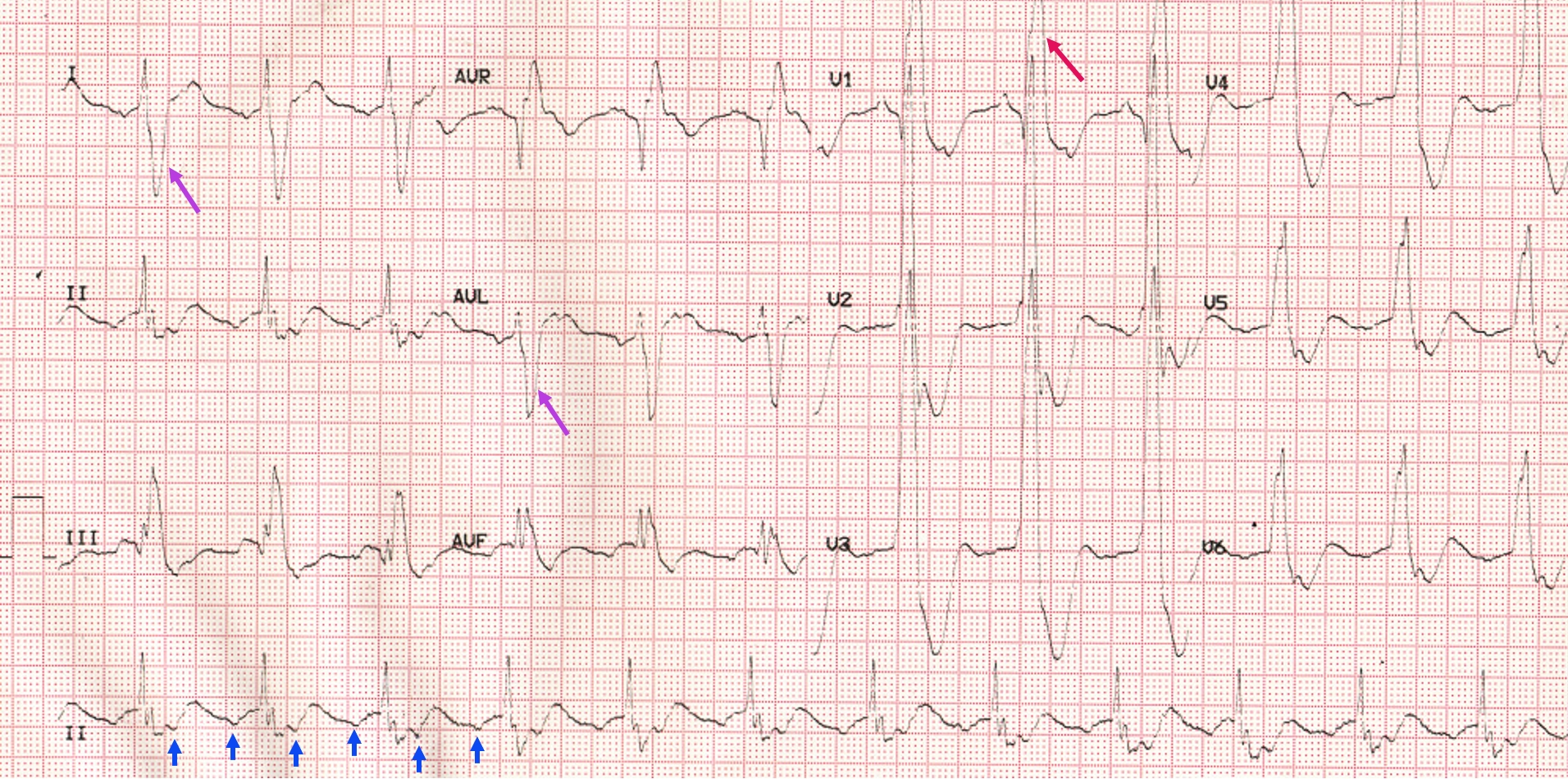
Here is an ECG which is typically seen in such cases of post repair TOF:
In early 70s, the cause of SCD was thought to be bradycardia due to atrioventricular (AV) block and bifascicular block was considered to be a risk factor. But later studies thought ventricular tachycardia (VT) to be the mechanism. Atrial flutter can also cause SCD, but final confirmation of its role is yet to come. Signal averaged ECGs for identifying late potentials have also been studied, but the results are variable. QT dispersion and JT dispersion have also been used for risk stratification.
Electrophysiology (EP) study may be useful for risk stratification being more sensitive but not really specific in predicting SCD. Left ventricular dysfunction is also an important risk factor of SCD. Yearly surveillance with ECG and echo and occasionally an MRI are needed. Those with severe pulmonary regurgitation and dilated right ventricle need pulmonary valve replacement. QRS width more than 180 ms calls for a cardiac catheterization and electrophysiology study.
References
- Gatzoulis MA, Till JA, Somerville J, Redington AN. Mechanoelectrical interaction in tetralogy of Fallot. QRS prolongation relates to right ventricular size and predicts malignant ventricular arrhythmias and sudden death. Circulation. 1995 Jul 15;92(2):231-7.
- Shiraishi S, Takahashi M, Sugimoto A, Tsuchida M. Predictors of ventricular tachyarrhythmia occurring late after intracardiac repair of tetralogy of Fallot: combination of QRS duration change rate and tricuspid regurgitation pressure gradient. J Thorac Dis. 2017 Dec;9(12):5112-5119.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal