Sleep apnea and cardiovascular disease
Sleep apnea and cardiovascular disease
Sleep-related breathing disorders are common in persons with cardiovascular disorders. Obstructive sleep apnea (OSA) is associated with hypertension, coronary artery disease, stroke and atrial fibrillation. The other variety of sleep apnea, namely central sleep apnea (CSA) occurs mainly in those with heart failure. It will be of great interest to know whether sleep apnea is the cause or effect of cardiovascular disease and whether sleep apnea can enhance the frequency of cardiovascular events. Another aspect which needs evaluation is on how much the treatment of sleep apnea can reduce these events.
Obstructive sleep apnea is due to the collapse of the pharyngeal airway during sleep. This obstruction could be partial causing hypopnea or complete, causing apnea. Apnea hypopnea index (AHI) is the number of episodes during an hour, with each episode lasting > 10 seconds. An AHI more than 5 is significant. The pharyngeal airway does not collapse in the awake state due to reflex activation of dilator muscles. This reflex is lost during sleep. But hypercapnia due to the apnea during sleep can stimulate the respiratory drive and cause arousal to activate the reflex. Obstructive sleep apnea is associated with snoring and increased day time somnolence.
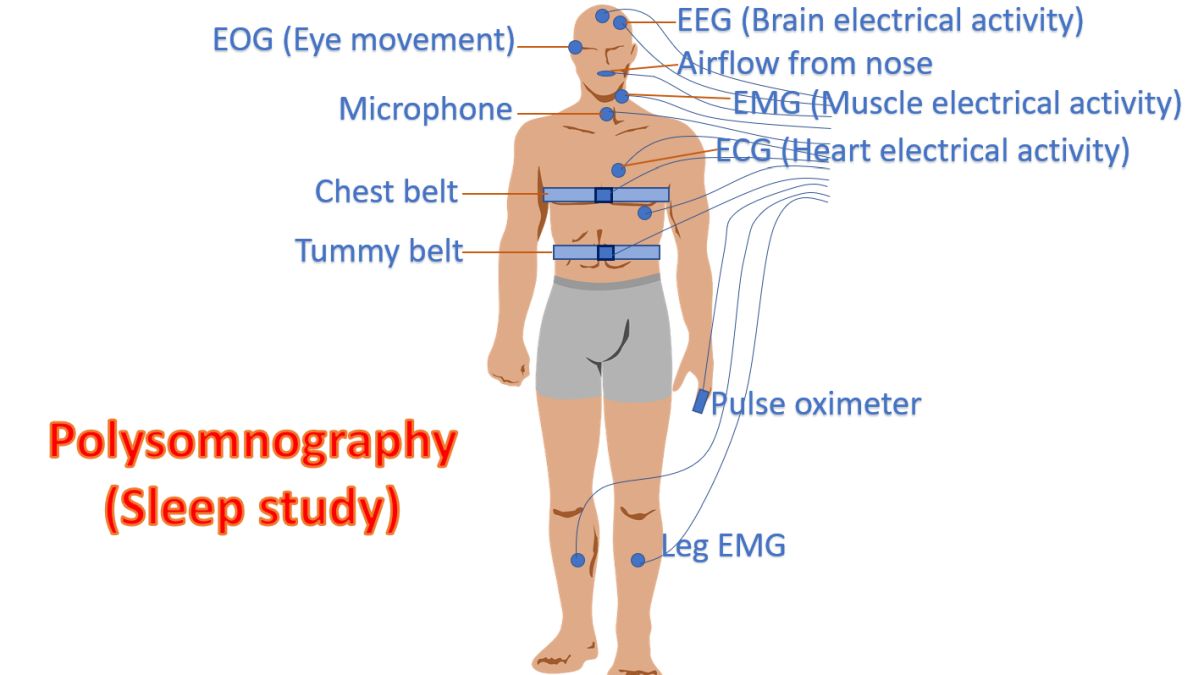
Definitive diagnosis of obstructive sleep apnea is done with a sleep study in a sleep laboratory with polysomnography. This involves electroencephalography to stage the sleep, electrooculogram to document eye movements to differentiate REM (rapid eye movement) and NREM sleep. A nasal thermistor monitors the respiration. Oxygen saturation and respiratory effort as well as flow are documented. Continuous ECG monitoring is also done as part of polysomnography.
Apneic episodes can be associated with severe rise in blood pressure even up to levels of 240/130 mm Hg. This is associated with hypoxia, hypercapnia and adrenergic activation in obstructive sleep apnea and can promote cardiovascular disease. Heart rate variability is reduced in those with obstructive sleep apnea. There is also release of endothelin which could be reduced by giving continuous positive airway pressure (CPAP). Oxidative stress and platelet activation also can occur in obstructive sleep apnea. Systemic inflammation with elevated C-reactive protein and endothelial dysfunction have been thought to be due to repeated episodes of apnea. Cardiac arrhythmias have also been correlated with episodes of obstructive sleep apnea. Apnea and hypoxemia have been thought to initiate bradyarrhythmias by eliciting the dive reflex causing vagal activation. Atrial fibrillation and ventricular premature complexes have been associated. Though there were initial reports of benefits from atrial pacing in sleep apnea, this was not demonstrated in subsequent studies. Other associations due to hypoxia are nocturnal angina, pulmonary hypertension and renal disease [1].
Reference
- Somers VK, White DP, Amin R, Abraham WT, Costa F, Culebras A, Daniels S, Floras JS, Hunt CE, Olson LJ, Pickering TG, Russell R, Woo M, Young T. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. J Am Coll Cardiol. 2008 Aug 19;52(8):686-717.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal