Transposition of great arteries
Transposition of great arteries
In transposition of great arteries (TGA), pulmonary artery arises from the left ventricle and aorta arises from the right ventricle. Aorta is anterior and to the right of pulmonary artery in D-TGA, which is the variety which we mean when we say just transposition of great arteries. L-TGA is a physiological corrected transposition with aorta to the left of the pulmonary artery, also called C-TGA. In L-TGA, in addition to ventricular arterial discordance, there is also atrioventricular discordance so that systemic venous blood flows from the right atrium to the morphological left ventricle and to the pulmonary artery. Similarly pulmonary venous flow reaches the morphological right ventricle from the left atrium and further into the aorta.
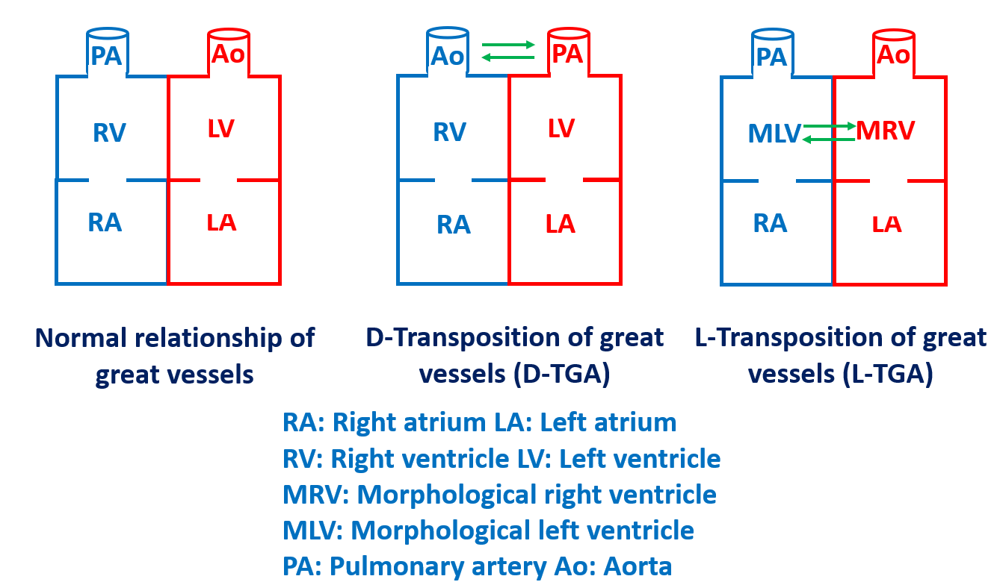
Here is a diagram showing the comparison between normally related great vessels, D-transposition of great arteries and corrected transposition of great arteries. The transposed ventricles in L-TGA are called morphological right ventricle and morphological left ventricle as they are situated on the opposite side.
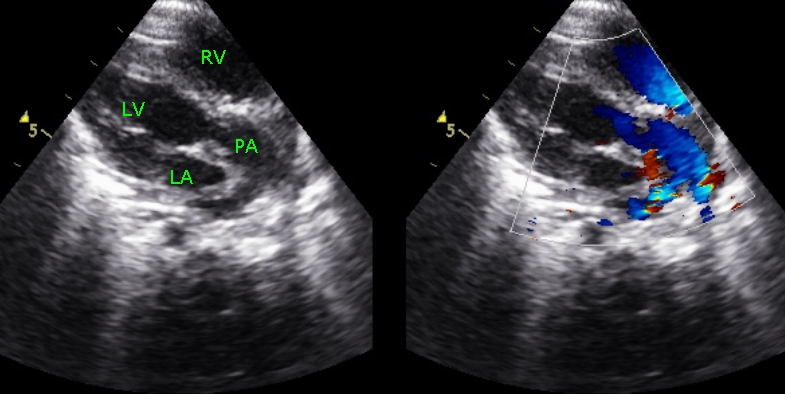
Echocardiogram in modified parasternal long axis view showing the vessel arising from the left ventricle bifurcating distally. It is pulmonary artery from left ventricle and hence transposition of great arteries. Aorta will not bifurcate and will show arch vessels when traced distally. Aorta was seen arising from the right ventricle in this cyanosed infant in another view.
In D-TGA, initial treatment is to have the ductus patent by prostaglandin infusion and further improve systemic saturation by balloon atrial septostomy. Atrial switch repair is known as Mustard procedure in which superior and inferior vena caval blood is baffled to the left atrium and onto the left ventricle and pulmonary artery. Pulmonary venous flow is baffled to the right atrium, right ventricle and the aorta. Symptom free survival until 2nd-3rd decade of life is feasible with Mustard procedure. The better option if diagnosed early in the neonatal period is an arterial switch operation or Jatene procedure. Long term data on arterial switch operation is being reported now. Competence of the pulmonic valve which becomes the neo-aortic valve is a question. Development of ostial stenosis in the reimplanted coronaries is also a concern. Long term complications of atrial based repair include arrhythmias and sudden cardiac death. Only eighteen percent maintain sinus rhythm and most go on to develop sick sinus syndrome atrial flutter/fibrillation and implantation of a permanent pacemaker may be needed in some. Systemic (tricuspid) atrioventricular valve regurgitation can develop in some. Whether tricuspid valve replacement is the final answer for this is not yet known. Systemic (RV) ventricular failure is another important problem. 15% have symptoms of heart failure by 2nd-3rd decade. Cardiac transplant or staged arterial switch with pulmonary banding to “train” the left ventricle may be an option in this case. Baffle obstructions are a rare (5%) but serious complication. Systemic venous obstruction is more common and should be suspected if new upper extremity edema develops. Pulmonary venous obstruction will manifest with new onset heart failure symptoms. Echocardiogram or cardiac catheterization is needed for further evaluation. Pulmonary venous obstruction can be treated surgically. Systemic venous obstruction may be treated with angioplasty/stents.
Most cases of L-TGA are asymptomatic for many years, often into adult life. Even though it is a physiologically corrected state, studies have shown that one fourth may die by a mean age of thirty eight years. Progressive heart failure, sudden cardiac death, AV block and atrial arrhythmias may occur in them. Severe tricuspid valve regurgitation requiring tricuspid valve replacement may occur. It may be difficult to image using echocardiograms and MRI may be needed, more so for better evaluation of right ventricular function.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal