Very wide QRS complex
Very wide QRS complex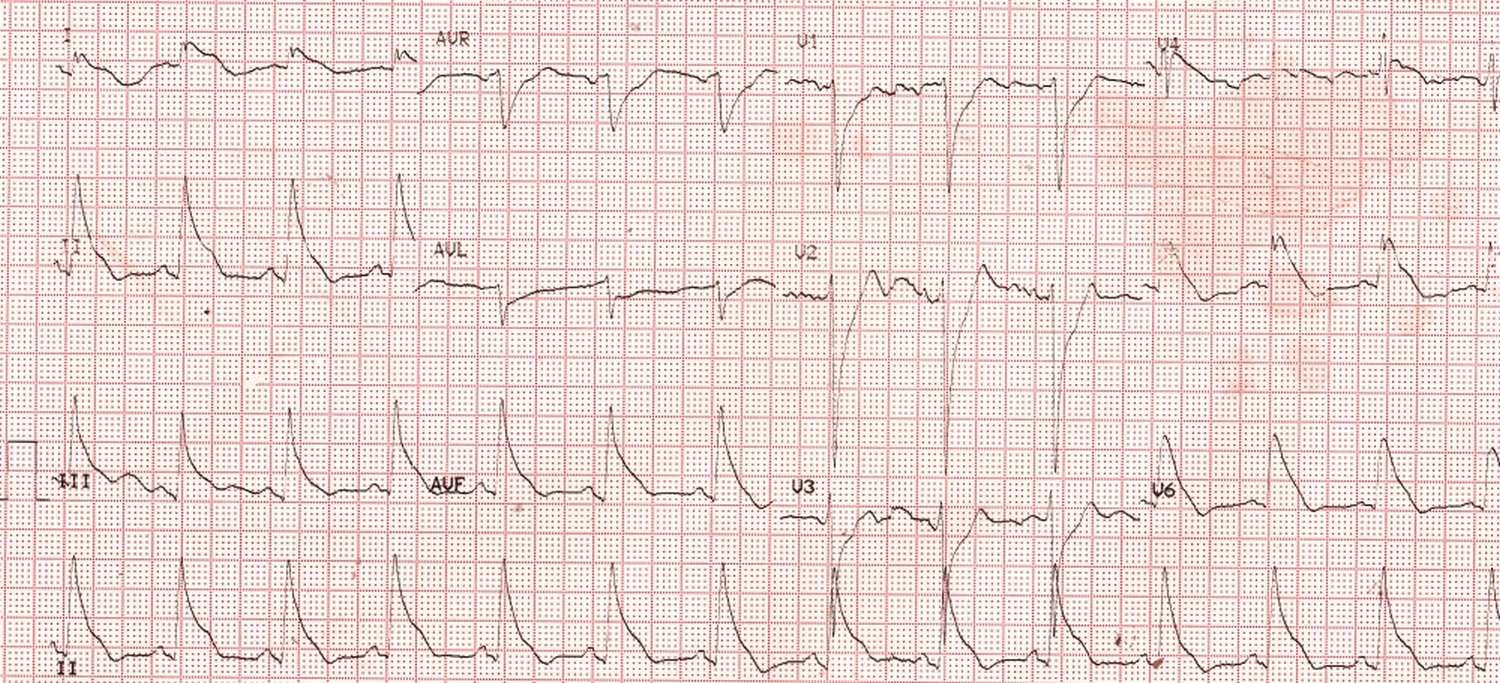
Width of the QRS complex in this ECG is about 200 ms. It is so wide that there is hardly any ST segment visible. The QRS merges into the T wave. One situation in which this occurs is severe hyperkalemia. But here the T waves are not tall and P waves are of reasonable amplitude, both against severe hyperkalemia. In severe hyperkalemia, P waves are flattened and disappear resulting in the so called sinoventricular conduction. Wide QRS in hyperkalemia merges with the tall T waves, producing a sine wave pattern, which is also absent here.
Initial upstroke of the QRS is sharp in this ECG while the terminal slurring is very prominent. In general, there is a left bundle branch block pattern, with positive QRS complex in lateral leads and negative QRS complex in anterior leads. This pattern can occur in severe heart failure and could be an indication for cardiac resynchronization therapy. In patients with heart failure and wide QRS complex, the mortality is double that of those with narrow QRS complex, thereby indicating more severe myocardial damage.
When the QRS complex is 200 ms or more the defibrillation threshold has been shown to be higher during implantable cardioverter defibrillator implantation [1]. Technical defect in the electrocardiograph should also be considered when bizarre QRS complexes are noted. But here the standardization pulse shows a perfect pattern and so are the P waves. Hence technical error is unlikely in this ECG.
Reference
- Kashani A, Barold S. Significance of QRS Complex Duration in Patients With Heart Failure. J Am Coll Cardiol. 2005;46(12):2183-2192.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal