X-ray Chest PA View
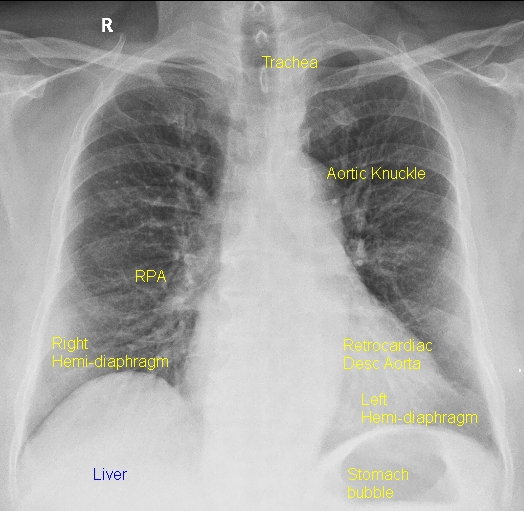
X-ray chest PA view gives a good assessment of the cardiac size. It is taken with the film in front of the chest and the X-ray tube behind, from a distance of 6 feet. This view avoids magnification of the heart as the film is close to the anterior chest wall. PA view is identified by the presence of the fundal gas bubble and the absence of the scapulae in the lung fields. Side of the liver shadow gives a hint to the situs, being solitus if it is on the right side.
The left cardiac border is formed by the aortic knuckle, pulmonary bay, left atrial appendage and left ventricle from above downwards. Right border is formed mostly by the right atrium, while a small portion of the inferior vena cava and superior vena cava may be seen. Ascending aorta may form the right upper border, especially if it is dilated. Indentation of the tracheal air shadow on the left side by the aortic arch indicates a left sided arch and vice versa.
Though the most commonly used projection for chest X-ray on an outpatient basis is PA view, almost all of the chest X-rays in the intensive care units are taken in the antero-posterior projection as the patient is often quite sick and unable to sit or stand. The cassette containing the X-ray film is placed behind the back of the patient in the bed. Of course there is no ‘film’ for a digital X-ray system. Instead there is an x-ray sensitive plate which can transfer the image data to a computer.
Occasionally a PA view in sitting posture is possible in the not so sick patients. AP view has a lot of limitations in assessing the cardiac structures. AP view introduces magnification of cardiac silhouette and apparent cardiomegaly is common. Widening of pedicle may be noted in supine view taken in the AP projection.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal