ASD overview and secundum ASD
ASD overview and secundum ASD
Atrial septal defect (ASD) is the commonest congenital heart disease in the adult, barring of course bicuspid aortic valve. ASD being a post tricuspid shunt, development of pulmonary hypertension and Eisenmenger syndrome is delayed and survival to adult age group is common. Some even argue that pulmonary hypertension in ASD is primary pulmonary hypertension which the individual was otherwise destined to develop. Anyway pulmonary hypertension is likely to develop in ASD with large left to right shunt of long duration, though the severity of pulmonary hypertension is variable. Supra systemic pulmonary arterial pressures are possible in pre tricuspid shunts like ASD unlike in VSD where the pressure can go only up to systemic levels. This is because the pressure in both ventricles get equalized in the presence of an unrestricted VSD. Usual types of ASD are the commonest ostium secundum ASD and the less common varieties of ostium primum ASD and sinus venosus ASD. Sinus venosus ASD can be subdivided into superior vena cava type and inferior vena cava type. The former is associated with partial anomalous venous drainage of the right sided pulmonary veins to the junction of superior vena cava and right atrium. Another type of ASD is the coronary sinus type of defect near the opening of the coronary sinus.
Secundum atrial septal defect
Secundum ASD in the region of the fossa ovalis. There is usually a good rim of tissue all around, making it suitable for device closure. Sometimes there can be multiple defects or a sieve like interatrial septum, which is difficult to close with a device. An interatrial septal aneurysm may be seen with a small defect at its apex. There is hardly any gradient between the atria in a large ASD and the left to right shunt is due to the higher compliance of the right ventricle compared to the left ventricle. At birth the right ventricle is dominant and the compliance is low. Hence the shunt in atrial septal defect is well established only when the right ventricle regresses. This is why ASD used to be detected late compared to VSD earlier. But now with ubiquitous availability of echocardiography, ASDs are often detected early in life. Bimodal pattern of cyanosis has been described in ASD, with mild cyanosis due to transient right to left shunt in early life with resolution and reappearance much later with the development of pulmonary hypertension and Eisenmenger reaction. Secundum ASDs can be familial and associated with first degree AV block.
Spontaneous closure of ASD: In the earlier era, since detection of atrial septal defects were delayed, it was thought that they seldom close spontaneously. Now with more frequent early detection of ASD with echocardiography in infancy, more and more cases of spontaneous closure have been reported. Smaller size of defect and early age of diagnosis, are important predictors of spontaneous closure. ASDs of less than 3 mm size diagnosed before 3 months of age are expected to close spontaneously. Though ASDs more than 8 mm in diameter are unlikely to close, case is on record in which 10 mm secundum ASD closed spontaneously within 1 year. There are reports of decrease in size of ASD without complete closure as well as reports of increase in size of ASD over time.
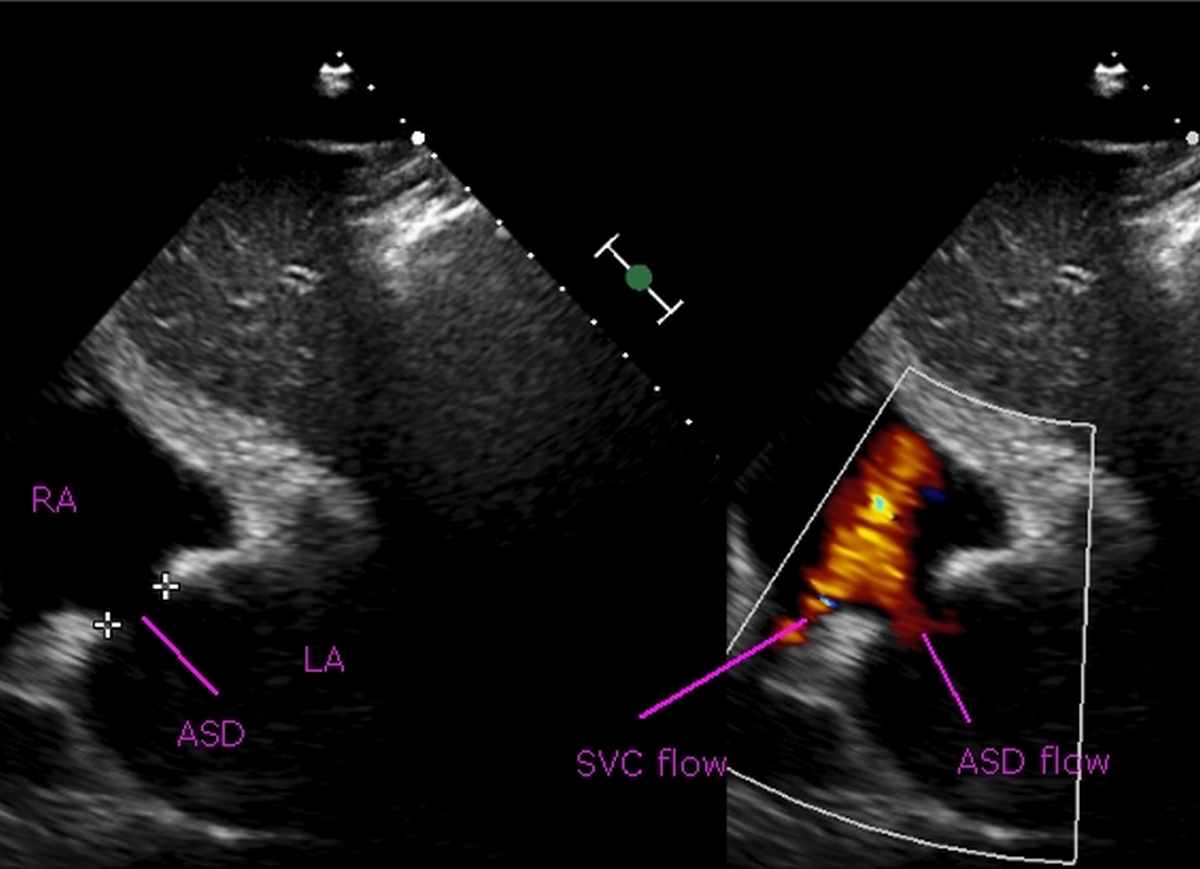
Subcostal view showing a 15 mm ASD on color Doppler echocardiogram. Left to right shunt (red color) is seen across the ASD in the right panel. RA: Right atrium, LA: Left atrium, SVC: Superior vena cava.
Transient right to left shunt can occur even without severe pulmonary hypertension due to phasic fluctuation of atrial pressures with respiration and Valsalva maneuver. Such right to left shunts can cause stroke due to paradoxical embolism (embolus from right side of heart reaching the left side of the heart and systemic circulation).
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal